Endoscopic Suturectomy
A Minimally Invasive Option for Craniosynostosis Treatment
For parents facing a diagnosis of craniosynostosis, the decision about which surgical approach is best for their child can feel overwhelming. Traditional open surgery, known as cranial vault remodeling (CVR), has been the standard treatment for decades. However, endoscopic suturectomy has emerged as a minimally invasive alternative that, for the right candidate, can offer excellent outcomes with a shorter surgery, less blood loss, and a faster recovery. This technique, when combined with postoperative helmet therapy, allows a baby’s skull to reshape naturally as it grows.
Understanding how endoscopic suturectomy works, who qualifies, and what the recovery process involves can help parents make an informed decision alongside their craniofacial specialist. Unlike open surgery, which involves large incisions and the immediate reconstruction of the skull, endoscopic suturectomy relies on the body’s natural growth process. By removing the fused suture through small incisions, the procedure allows the skull to expand in the proper direction over time. This method works best when performed very early in infancy, usually before three months of age, when the skull is still flexible and able to be guided by a custom helmet worn for several months after surgery.
This page will explain who is a good candidate for endoscopic suturectomy, what happens during surgery, and what parents should expect before, during, and after the procedure. It will also explore how helmet therapy plays a critical role in ensuring the best results, as well as how this approach compares to traditional surgery. By the end, parents will have a clear understanding of whether this minimally invasive procedure might be the right choice for their child.
Endoscopic Suturectomy
A Minimally Invasive Option for Craniosynostosis Treatment

Table Of Contents
Indications & Patient Selection
Endoscopic suturectomy is a highly effective treatment for craniosynostosis, but it is not the right option for every child. Unlike traditional open surgery, which can be performed later in infancy, this minimally invasive approach relies on the skull’s natural ability to reshape during early growth. The timing of the procedure and the specific type of craniosynostosis will determine whether your child is a good candidate. Understanding the selection criteria can help you decide whether this procedure is the best choice for your baby.
Another important consideration is parental commitment to helmet therapy. Unlike traditional surgery, where the surgeon immediately reshapes the skull during the procedure, endoscopic suturectomy relies on months of guided skull growth with a specially designed helmet. Families who are unable to commit to strict helmet therapy (23 hours per day for 6-12 months) may not see optimal results, making open surgery a more predictable option.

Ideal Candidates for Endoscopic Suturectomy
- Sagittal
- Metopic
- Unilateral Coronal
- Lambdoid
- Syndromic
Metopic
- Overview
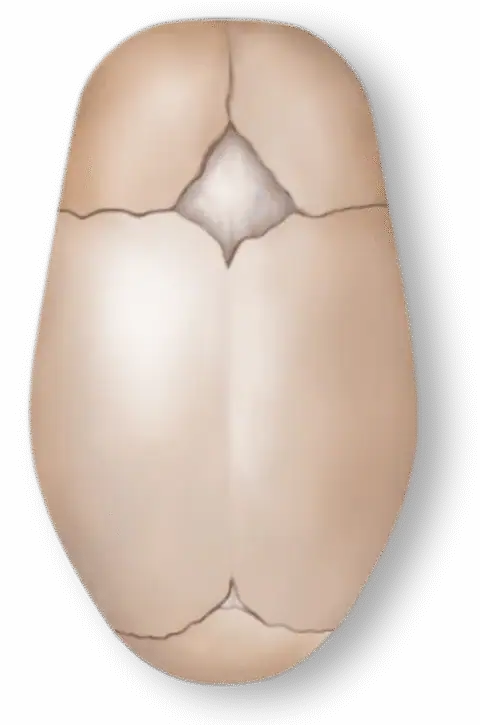
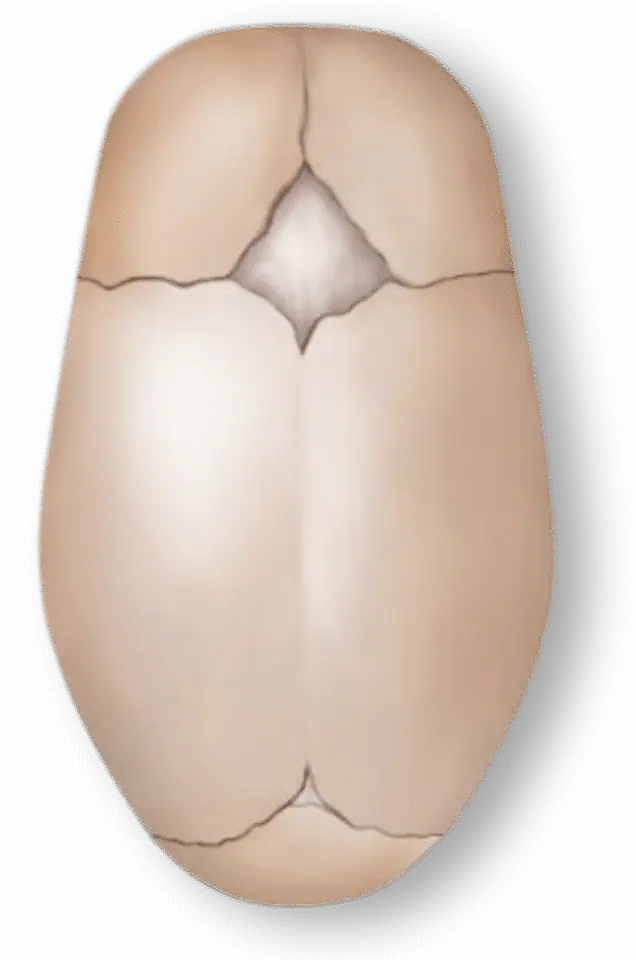
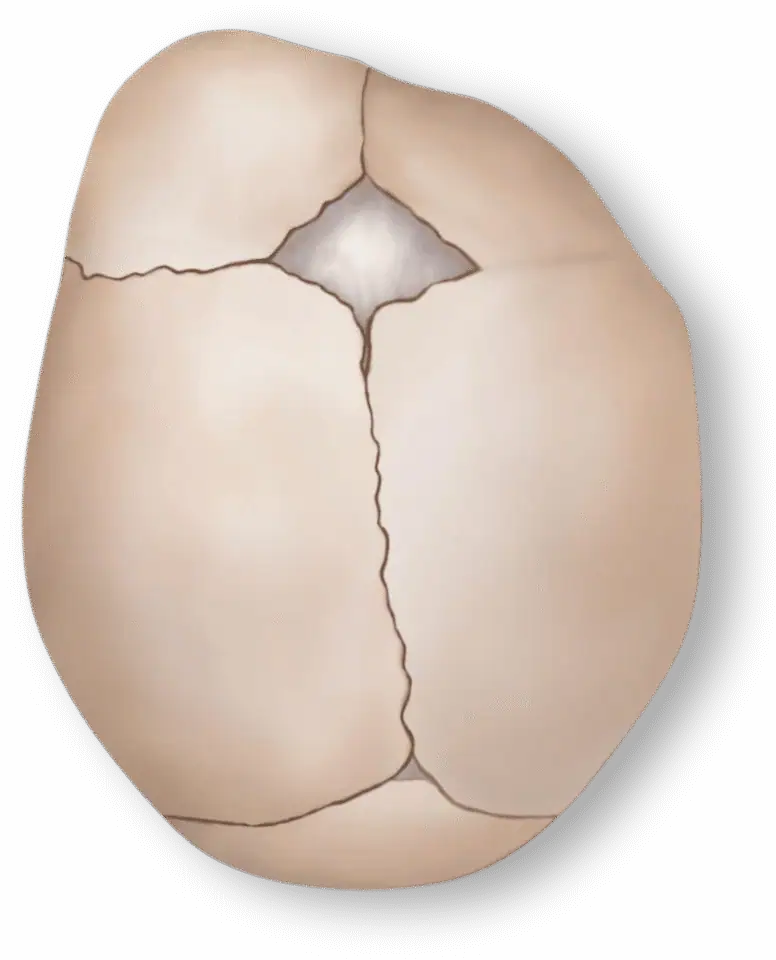
This is the most common type of single-suture craniosynostosis, where the sagittal suture (running from front to back along the top of the head) fuses prematurely, causing an elongated skull.
Endoscopic release allows the head to widen over time with helmet therapy.
The overall incidence of Craniosynostosis is approximately 1 in 2000/3000 births. Metopic synostosis is relatively rare, accounting for between 5% and 15% of all craniosynostosis cases.
Diagnostically, the condition can be identified through a physical examination, where the triangular shape of the forehead and ridging are noticeable. Imaging techniques, such as computed tomography (CT) scans, can confirm the diagnosis and assess the extent of the fusion.
Treatment typically involves surgery to correct the skull shape and allow for normal brain growth. The surgical procedure, usually performed in the first year of life, involves removing and reshaping the fused bones to create a more typical skull contour. Please refer to our Treatment Options page for a more detailed explanation of these surgical procedures.
Coronal
- Overview
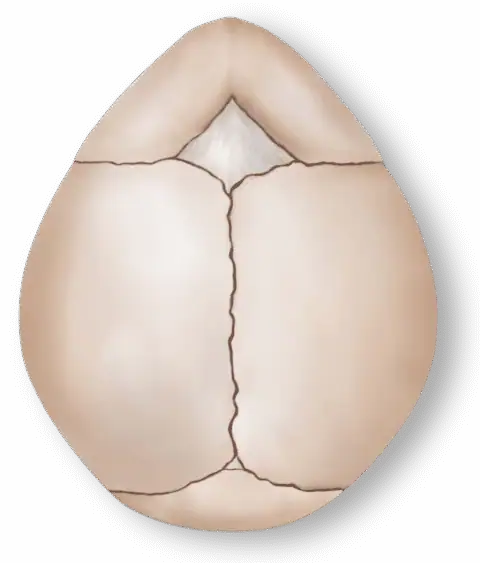
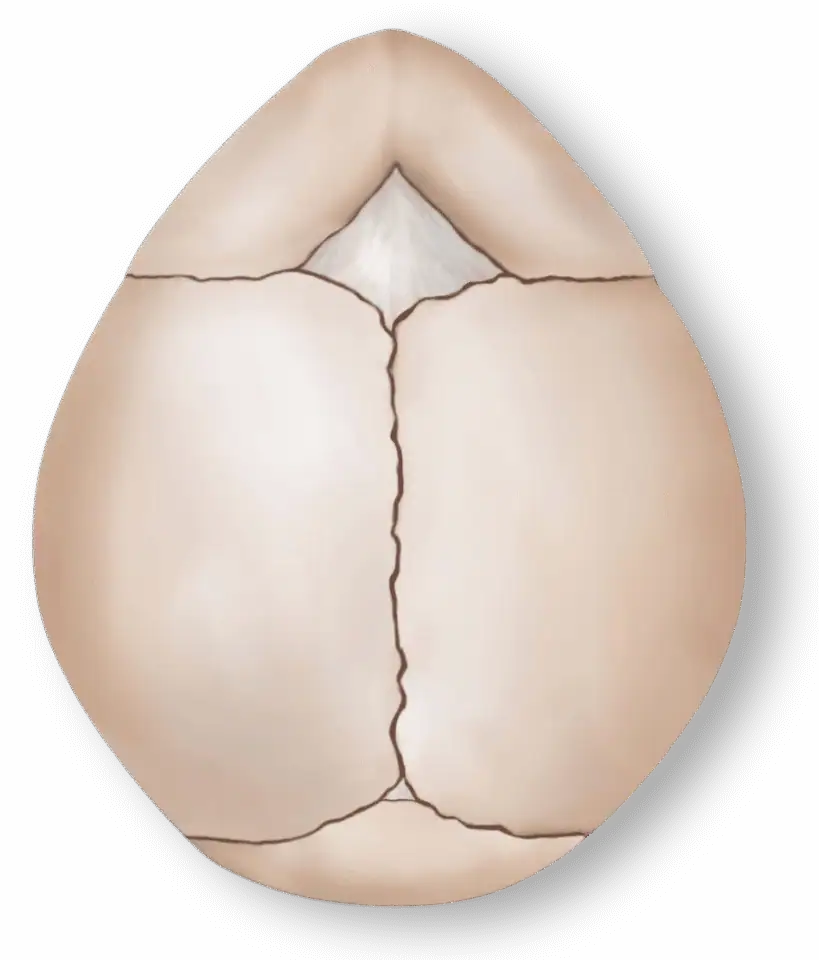
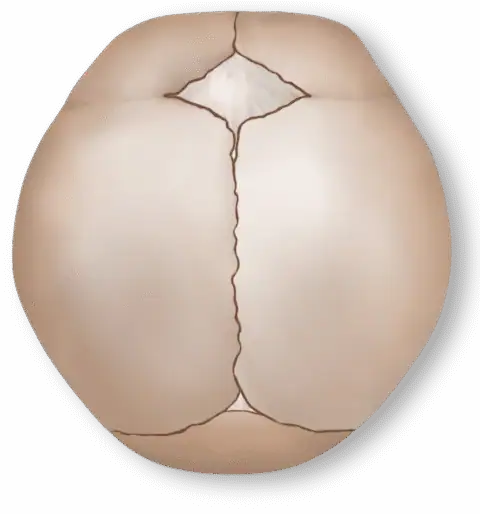
Premature closure of the metopic suture (running from the forehead to the top of the skull) results in a triangular-shaped forehead. In mild to moderate cases, endoscopic suturectomy may allow for gradual correction. However, more severe cases may still require open surgery.
The overall incidence of Craniosynostosis is approximately 1 in 2000/3000 births. Metopic synostosis is relatively rare, accounting for between 5% and 15% of all craniosynostosis cases.
Diagnostically, the condition can be identified through a physical examination, where the triangular shape of the forehead and ridging are noticeable. Imaging techniques, such as computed tomography (CT) scans, can confirm the diagnosis and assess the extent of the fusion.
Treatment typically involves surgery to correct the skull shape and allow for normal brain growth. The surgical procedure, usually performed in the first year of life, involves removing and reshaping the fused bones to create a more typical skull contour. Please refer to our Treatment Options page for a more detailed explanation of these surgical procedures.
Sagittal
- Overview
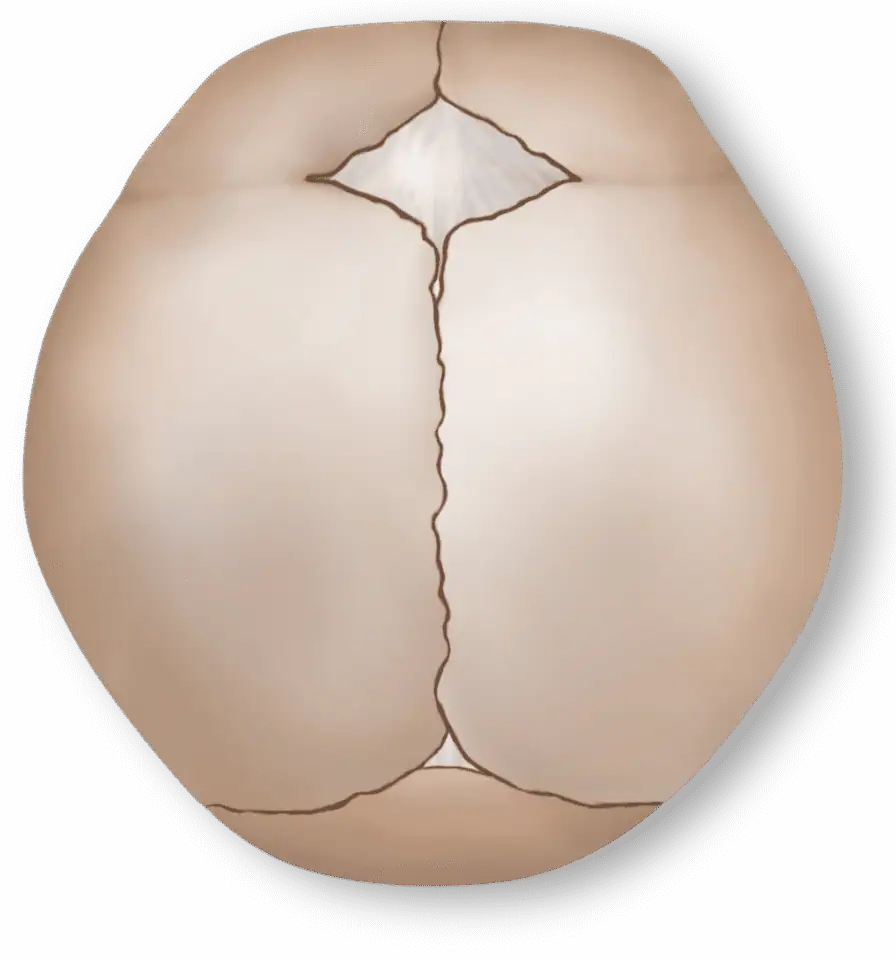
Fusion of one coronal suture (running from the ear to the top of the head) leads to forehead flattening and orbital asymmetry. Endoscopic release can be effective if diagnosed early, but helmet therapy is crucial for guiding correction.

The overall incidence of Craniosynostosis is approximately 1 in 2000/3000 births. Metopic synostosis is relatively rare, accounting for between 5% and 15% of all craniosynostosis cases.
Diagnostically, the condition can be identified through a physical examination, where the triangular shape of the forehead and ridging are noticeable. Imaging techniques, such as computed tomography (CT) scans, can confirm the diagnosis and assess the extent of the fusion.
Treatment typically involves surgery to correct the skull shape and allow for normal brain growth. The surgical procedure, usually performed in the first year of life, involves removing and reshaping the fused bones to create a more typical skull contour. Please refer to our Treatment Options page for a more detailed explanation of these surgical procedures.
Sagittal
- Overview
Fusion of the lambdoid suture (at the back of the skull) causes a flattened appearance on one side. This type is less common, but when caught early, endoscopic treatment may provide good results.

The overall incidence of Craniosynostosis is approximately 1 in 2000/3000 births. Metopic synostosis is relatively rare, accounting for between 5% and 15% of all craniosynostosis cases.
Diagnostically, the condition can be identified through a physical examination, where the triangular shape of the forehead and ridging are noticeable. Imaging techniques, such as computed tomography (CT) scans, can confirm the diagnosis and assess the extent of the fusion.
Treatment typically involves surgery to correct the skull shape and allow for normal brain growth. The surgical procedure, usually performed in the first year of life, involves removing and reshaping the fused bones to create a more typical skull contour. Please refer to our Treatment Options page for a more detailed explanation of these surgical procedures.
Lambdoid
- Overview
For babies with multiple fused sutures or syndromic craniosynostosis (such as Apert, Crouzon, or Pfeiffer syndromes), endoscopic suturectomy is typically not the primary treatment, as these cases often require a more extensive reconstruction to relieve intracranial pressure and reshape the skull. However, in select cases, an endoscopic procedure may be used as a first-stage surgery to relieve pressure before a more extensive reconstruction is performed later in childhood.
The overall incidence of Craniosynostosis is approximately 1 in 2000/3000 births. Metopic synostosis is relatively rare, accounting for between 5% and 15% of all craniosynostosis cases.
Diagnostically, the condition can be identified through a physical examination, where the triangular shape of the forehead and ridging are noticeable. Imaging techniques, such as computed tomography (CT) scans, can confirm the diagnosis and assess the extent of the fusion.
Treatment typically involves surgery to correct the skull shape and allow for normal brain growth. The surgical procedure, usually performed in the first year of life, involves removing and reshaping the fused bones to create a more typical skull contour. Please refer to our Treatment Options page for a more detailed explanation of these surgical procedures.
Making the Right Decision
Choosing the right treatment for craniosynostosis is a deeply personal decision that depends on your baby’s age, the severity of the condition, and your family’s commitment to following through with postoperative care. When diagnosed early, endoscopic suturectomy offers a minimally invasive way to correct craniosynostosis with less pain, a faster recovery, and excellent long-term results. However, for families seeking immediate correction without the need for helmet therapy, or for cases where the condition is more complex, cranial vault remodeling may be the better choice.
By working closely with a craniofacial specialist, you can determine whether your child is a good candidate for this approach and what to expect in the weeks and months following surgery. In the next sections, we will take a closer look at the preoperative evaluation process and the procedure itself to give you a clear understanding of what to expect throughout the process.


Preoperative Evaluation
Once a baby has been identified as a candidate for endoscopic suturectomy, the next step is a thorough preoperative evaluation. This stage ensures that the child is healthy enough for surgery, confirms the diagnosis and severity of craniosynostosis, and prepares both the medical team and parents for what to expect before, during, and after the procedure. Unlike open cranial vault surgery, which involves a more extensive reshaping of the skull, endoscopic suturectomy relies on early intervention and guided growth. Because of this, timing and careful planning are essential to achieving the best outcome.
A successful evaluation involves several key components, including a clinical examination, imaging studies, and coordination with a multidisciplinary team. You will also meet with your surgeon and other specialists who will be involved in your child’s care. This is an important time to ask any lingering questions, discuss the logistics of the surgery and helmet therapy, and ensure that your family is prepared for the process ahead.
Parental Preparation: What to Expect Before Surgery
Preoperative Checkups
A final physical exam, blood tests, and anesthesia evaluation to confirm your child is fit for surgery
Feeding Guidelines
Instructions on when to stop feeding before surgery, usually several hours to prevent complications under anesthesia
Helmet Therapy Consultation
A meeting with a cranial orthotist to discuss how and when the helmet will be fitted postoperatively
A Reassuring Overview
Many parents feel anxious about their baby undergoing surgery, even if it is minimally invasive. It can be reassuring to remember that endoscopic suturectomy has a high success rate, a short hospital stay, and a fast recovery compared to open surgery. Understanding what to expect can help ease concerns and make the experience feel more manageable.


The Endoscopic Suturectomy Procedure
On the day of surgery, you may feel a mix of emotions—hope, nervousness, and a strong desire to ensure your baby is receiving the best possible care. While endoscopic suturectomy is a minimally invasive procedure, understanding exactly what happens during surgery, how long it takes, and what to expect afterward can provide reassurance. Unlike traditional cranial vault remodeling, which involves extensive skull reshaping and longer recovery times, this approach focuses on removing the fused suture with minimal disruption to the surrounding bone, allowing the skull to reshape naturally with the help of helmet therapy.
This section will walk you through the entire surgical process—from arrival at the hospital to the procedure itself and the immediate recovery period. Knowing what to expect can help you feel prepared and confident as you support your child through this important step in treatment.
Arriving at the Hospital & Pre-Surgical Preparation
Morning of Surgery
On the morning of surgery, you and your baby will arrive at the hospital a few hours before the scheduled procedure. This allows time for final preoperative checks and for you to meet with the surgical and anesthesia teams.
Medical Review
The surgical team will confirm your baby’s weight, vital signs, and recent health history to ensure there are no last-minute concerns.
Anesthesia Consultation
The pediatric anesthesiologist will explain how sedation will be administered and answer any questions you may have. Since babies are under general anesthesia for the procedure, they are asleep and pain-free throughout.
Marking the Surgical Site
The surgeon may make small markings on your baby’s scalp to indicate incision sites.
Parental Goodbye & Transition to Surgery
You will be able to hold and comfort your baby before surgery begins. The medical team will then gently bring your baby into the operating room, where anesthesia will be administered.
It’s normal to feel emotional during this moment, but it may help to remember that this is a well-practiced, low-risk procedure performed by a highly experienced team. The actual surgery itself is relatively quick, typically lasting about one hour.

Step-by-Step Breakdown of the Surgery
1.
Positioning & Sterilization
- Your baby is carefully positioned, usually lying on their back, to provide the best access to the affected suture.
- The surgical area is cleaned and sterilized, and a small portion of the hair may be shaved near the incision sites.
2.
Creating the Small Incisions
- The surgeon makes two or three small incisions (about 1-2 cm each) over the fused suture.
- These incisions are made in locations that will heal well and be minimally visible over time.
3.
Using the Endoscope
- A tiny, camera-guided instrument called an endoscope is inserted through one incision. This allows the surgeon to see the fused suture with high precision while keeping the incisions as small as possible.
- Other small instruments are inserted through the additional incisions to carefully cut and remove the fused suture.
4.
Removing the Fused Suture
- Using specialized tools, the surgeon removes a strip of bone along the fused suture to create space for the skull to grow naturally.
- The amount of bone removed is typically 1-2 cm wide, just enough to release the restriction without affecting surrounding areas.
5.
Ensuring Safety
- Since the incisions are small, bleeding is usually minimal, but the surgeon takes extra care to seal small blood vessels as needed.
- The dura (the protective layer around the brain) is carefully preserved, and the skull is left intact aside from the removed suture.
6.
Closing the Incisions
- The surgeon closes the small incisions using dissolvable stitches or surgical glue. These will heal on their own over the next few weeks.
- No plates, screws, or artificial implants are needed, as the skull will reshape naturally with helmet therapy.
Immediate Postoperative Recovery

Pain Management
Since endoscopic suturectomy is less invasive than open surgery, pain is usually mild to moderate and managed with acetaminophen (Tylenol) or ibuprofen (Advil) rather than strong narcotics.
Swelling & Bruising
Some mild swelling or puffiness around the forehead and eyes is expected, but it is far less severe than with cranial vault remodeling. It typically peaks within 48 hours and resolves quickly.
Feeding & Comfort
Babies can usually resume breastfeeding or bottle-feeding within a few hours after surgery. You are encouraged to hold, comfort, and soothe your baby as soon as they are awake.
Helmet Therapy Planning
Before being discharged, you will receive instructions on when to visit the orthotist for helmet fitting (usually within 1-2 weeks).
Unlike traditional open surgery, which requires several days in the hospital, most babies go home the same day or after an overnight stay. You will receive detailed care instructions, including how to keep the incisions clean, what signs of infection to watch for, and when to follow up with the surgical team.
Helmet Therapy & Postoperative Management
The success of endoscopic suturectomy does not end in the operating room. Unlike traditional open surgery, where the skull is reshaped immediately, this minimally invasive approach relies on the baby’s natural growth to gradually correct head shape. Helmet therapy plays a critical role in ensuring the best possible cosmetic and functional outcomes.
Helmet therapy can feel like a big commitment—it requires consistent wear (23 hours per day) for several months and regular adjustments. However, when used correctly, it allows for a smooth and even expansion of the skull, helping the baby’s head grow into a normal, symmetrical shape. This section will explain how helmet therapy works, what to expect, and how to ensure the best results in the months following surgery.

Why is Helmet Therapy Necessary?

What happens after endoscopic suturectomy?
After endoscopic suturectomy, the removed suture leaves a gap, allowing the skull to grow in previously restricted areas. However, without guidance, the head may not expand evenly. The helmet provides a gentle but structured shape, ensuring that as the skull grows, it fills in the right areas while preventing unwanted flattening or irregularities.
Why Helmet Therapy is important?
Helmet therapy is especially important because babies’ skulls grow the fastest in the first year of life, meaning this is the ideal time to reshape the head naturally without additional surgery. Parents who are diligent about keeping their baby in the helmet for the recommended time typically see excellent results, often resulting in a near-normal head shape by the child’s first birthday.
Getting Started
When is the Helmet Fitted?
The first helmet fitting takes place about 1-2 weeks after surgery, once the incisions have healed enough to allow for safe wear. This timeline is important because early intervention ensures that skull growth is guided from the start, preventing deformities from developing.
During the initial fitting:
- A cranial orthotist (a specialist trained in cranial helmets) will take precise 3D measurements of your baby’s head.
- A custom-fitted cranial molding helmet will be designed to guide growth in the correct areas.
- You will be instructed on how to properly place, remove, and clean the helmet, as well as what to expect in terms of adjustments and follow-ups.
The first few days are a transitional period during which babies gradually increase their helmet-wearing time. Most infants adjust quickly and tolerate the helmet well, especially since it is lightweight, comfortable, and custom-fitted.
Helmet Wear Schedule & Adjustments
To achieve the best outcome, babies should wear the helmet 23 hours per day, removing it only for:
- Bathing
- Cleaning the helmet
- Skin checks (to ensure there is no irritation or redness)
The helmet does not squeeze or reshape the skull with pressure. Instead, it provides a guiding structure, allowing the skull to grow into the areas where space has been created.Because babies grow rapidly, regular helmet adjustments are necessary.
Follow-up appointments with the cranial orthotist are typically scheduled:- Every 2-4 weeks in the first few months
- Less frequently as skull growth slows
At these visits, the orthotist:- Checks head growth progress
- Modifies the helmet to ensure proper guidance
- Addresses any fit concerns
You will also have periodic follow-ups with the craniofacial surgeon to monitor the overall surgical outcome and ensure the skull is growing as expected.
How Long Will My Baby Need the Helmet?
The duration of helmet therapy depends on the age of your baby at the time of surgery, the type of suture used, and the rate of skull reshaping; however, most babies wear the helmet for 6-12 months:
- Younger infants (2-3 months old at the time of surgery) may require longer helmet therapy because their skulls have more growing to do.
- Older infants(closer to 4-5 months old) often complete therapy in a shorter time because their skulls grow at a slightly slower rate.
- The helmet is discontinued once the desired head shape is achieved and skull growth slows naturally (usually around 12-18 months of age).
What to Expect as Parents
At first, helmet therapy may feel like an adjustment, but most babies adapt quickly and do not seem to mind it. Parents, however, often have concerns about comfort, fit, and whether their baby will be bothered by the helmet.
Here’s what to expect:
- Most babies adjust within a few days and do not show signs of discomfort.
- Helmets are lightweight, well ventilated, and designed to keep babies cool.
- There is no pain involved—helmets guide natural growth rather than applying pressure.
- Daily cleaning is essential to prevent irritation from sweat and oils.
- Skin redness may occur but should fade quickly after removing the helmet for cleaning.
Parental commitment to helmet therapy is one of the most important factors in achieving the best results.
Staying consistent with wear time and follow-up visits ensures that the skull grows symmetrically and evenly, avoiding the need for additional interventions.
What Happens If Helmet Therapy is Not Followed?
If the helmet is not worn as prescribed, the skull may not reshape properly, leading to:
- Residual skull asymmetry (which may be permanent)
- Less effective correction of the craniosynostosis
- Potential need for additional procedures later in childhood
Since the goal of endoscopic suturectomy is to allow for natural skull reshaping, missing helmet therapy may result in incomplete treatment.
This is why parents play a critical role in ensuring their child gets the full benefits of surgery.

Outcomes &
Long-Term Results
For parents choosing endoscopic suturectomy, one of the most important questions is:
What kind of results can we expect?
The good news is that this minimally invasive approach provides excellent cosmetic and functional outcomes when performed early and followed by consistent helmet therapy.
Unlike traditional open surgery, which reshapes the skull immediately, endoscopic suturectomy allows the baby’s natural growth to do most of the work. As a result, improvements become more apparent over time, with the most significant changes occurring within the first 12-18 months after surgery.
By the time treatment is complete, most children have normal or near-normal head shapes and no long-term functional issues related to craniosynostosis.
Getting Started
Cosmetic Outcomes: How Well Does the Skull Reshape?
The primary goal of endoscopic suturectomy is to allow the skull to grow in a more natural shape while avoiding the more invasive nature of open surgery. Since helmet therapy guides this process, the final results are typically:
- Smooth, symmetrical head shape with improved proportions.
- Reduced forehead or back-of-head flattening, depending on the type of craniosynostosis.
- Better overall skull balance, with natural rounding over time.
- For most children, the head shape continues to improve gradually over the first two years of life, as growth slows and the skull takes on its final form.
It’s important to note that while helmet therapy helps achieve excellent results, perfection is not always the goal. Some children may still have slight asymmetries, but these are usually mild and not noticeable to others. In rare cases, if the reshaping is incomplete, additional treatment may be considered later in childhood.
Neurodevelopmental Outcomes: Does Surgery Affect Brain Growth?
One of the biggest concerns parents have is whether craniosynostosis or its treatment will impact brain development. Fortunately, studies show that when treated early, children who undergo endoscopic suturectomy develop normally, with no negative impact on intelligence, learning, or neurological function:
- The procedure removes the fused suture, allowing the skull to grow without restriction.
- There is no interference with the brain itself, as the surgery is performed only on the outer bone.
- Long-term research has demonstrated that children who undergo early treatment for craniosynostosis exhibit similar academic and cognitive development outcomes to their peers.
However, if craniosynostosis is left untreated, it can sometimes lead to increased intracranial pressure, which may contribute to headaches, vision problems, or developmental delays. This is why early diagnosis and treatment are so important—they help ensure healthy skull and brain development with no long-term concerns.Does Endoscopic Suturectomy Prevent the Need for Future Surgery?
For most children, one surgery is enough, and no further treatment is required. However, in a small percentage of cases (about 5-15%), additional surgery may be considered if:
- Helmet therapy was not followed correctly, leading to incomplete skull reshaping.
- The skull fuses in an unexpected way, limiting growth.
- New areas of flattening develop, requiring minor adjustments.
When additional treatment is needed, it is usually less invasive than a full cranial vault reconstruction. In some cases, minor adjustments can be made using a second helmet, bone grafting, or a small corrective procedure later in childhood.
However, with early intervention and proper helmet use, most children achieve excellent results with just one surgery.
Parental Satisfaction: What Do Families Think of Endoscopic Suturectomy?
Parents who choose endoscopic suturectomy often report high levels of satisfaction with their child’s results, especially because of the minimally invasive nature of the procedure. Some of the most commonly mentioned benefits include the following:
- Smaller scars that heal quickly and are barely noticeable over time.
- Shorter hospital stay and faster recovery compared to open surgery.
- Less swelling and discomfort after surgery.
- Excellent long-term head shape with helmet therapy.
The biggest challenge parents report is adapting to helmet therapy in the months following surgery. However, most families say that seeing the gradual improvements in their child’s head shape makes the commitment worthwhile. For parents who stay diligent with helmet use, the results are often just as good—or even better—than those achieved with open surgery.
Long-Term Follow-Up: What Happens After Treatment Ends?
After the helmet therapy phase is completed, most children only require routine follow-up visits with their craniofacial team to monitor skull growth over time:
- By 18-24 months of age, helmet therapy is typically discontinued, and the head shape is considered stable.
- By preschool age, most children show no visible signs of having had craniosynostosis, and their development is completely normal.
- In rare cases, minor refinements to the skull shape can be made later in childhood, but this is uncommon.
There are no long-term activity restrictions—children who have undergone endoscopic suturectomy can play sports, swim, and do everything other kids do. The skull bones fully heal and develop just as strong as any other child’s, meaning there is no increased risk of injury.
Comparing Endoscopic Suturectomy and Cranial Vault Remodeling
For parents exploring treatment options for craniosynostosis, one of the biggest decisions is choosing between endoscopic suturectomy and traditional CVR. Both surgeries aim to correct skull shape abnormalities and facilitate normal brain growth, but they take very different approaches.
Endoscopic suturectomy is minimally invasive, relying on early intervention and helmet therapy to guide natural skull growth. Cranial vault remodeling, on the other hand, is a more extensive procedure that immediately reshapes the skull and does not require helmet therapy afterward.
Each approach has its advantages, challenges, and ideal candidates, making it important for parents to understand which option best suits their child’s needs.

Key Differences Between Endoscopic Suturectomy & Cranial Vault Remodeling
| Feature | Endoscopic Suturectomy | Cranial Vault Remodeling (CVR) |
|---|---|---|
| Age Requirement | Performed before 3 months of age | Performed between 6–12 months |
| Surgical Approach | Minimally invasive (small incisions) | Open surgery (large incision across the scalp) |
| Procedure Time | About 1 hour | 3–5 hours |
| Blood Loss | Minimal, low chance of transfusion | Higher blood loss, higher chance of transfusion. |
| Hospital Stay | 1 day or overnight | 3–5 days |
| Recovery Time | Faster, minimal swelling | Longer, significant swelling |
| Helmet Therapy | Required for 6–12 months | Not required |
| Results Timeline | Gradual improvement over time | Immediate reshaping |
| Ideal case severity | Mild to moderate cases | Moderate to severe cases |
| Long-Term Outcomes | Excellent if helmet therapy is followed | Excellent, no helmet needed |
Age Requirement
- Endoscopic Suturectomy
Performed before 3 months of age - Cranial Vault Remodeling (CVR)
Performed between 6–12 months
- Endoscopic Suturectomy
Surgical Approach
- Endoscopic Suturectomy
Minimally invasive (small incisions) - Cranial Vault Remodeling (CVR)
Open surgery (large incision across the scalp)
- Endoscopic Suturectomy
Procedure Time
- Endoscopic Suturectomy
About 1 hour - Cranial Vault Remodeling (CVR)
3–5 hours
- Endoscopic Suturectomy
Blood Loss
- Endoscopic Suturectomy
Minimal, low chance of transfusion - Cranial Vault Remodeling (CVR)
Higher blood loss, higher chance of transfusion.
- Endoscopic Suturectomy
Hospital Stay
- Endoscopic Suturectomy
1 day or overnight - Cranial Vault Remodeling (CVR)
3–5 days
- Endoscopic Suturectomy
Recovery Time
- Endoscopic Suturectomy
Faster, minimal swelling - Cranial Vault Remodeling (CVR)
Longer, significant swelling
- Endoscopic Suturectomy
Helmet Therapy
- Endoscopic Suturectomy
Required for 6–12 months - Cranial Vault Remodeling (CVR)
Not required
- Endoscopic Suturectomy
Results Timeline
- Endoscopic Suturectomy
Gradual improvement over time - Cranial Vault Remodeling (CVR)
Immediate reshaping
- Endoscopic Suturectomy
Ideal case severity
- Endoscopic Suturectomy
Mild to moderate cases - Cranial Vault Remodeling (CVR)
Moderate to severe cases
- Endoscopic Suturectomy
Long-Term Outcomes
- Endoscopic Suturectomy
Excellent if helmet therapy is followed - Cranial Vault Remodeling (CVR)
Excellent, no helmet needed
- Endoscopic Suturectomy
Advantages of Endoscopic Suturectomy

Endoscopic suturectomy is ideal for parents who prefer a less invasive option and can commit to helmet therapy. Here are some of the most significant benefits of endoscopic suturectomy:
- Minimally invasive: Smaller incisions result in less scarring and quicker healing.
- Shorter hospital stay: Most babies go home the same day or after an overnight stay.
- Lower risk of complications: There is less blood loss, reduced swelling, and a faster recovery compared to open surgery.
- More natural skull growth: Instead of an immediate reshaping, the skull gradually expands into the correct shape over time.
- Helmet therapy allows for a more controlled and guided reshaping of the skull.
However, helmet therapy is a critical part of the process. Parents must be fully prepared to follow the helmet wear schedule (23 hours per day for 6-12 months) to ensure successful results.
Advantages of Cranial Vault Remodeling (CVR)
Immediate skull reshaping
The skull is fully corrected in the operating room, so parents see results immediately.
Better for severe cases
If the skull deformity is more complex, CVR allows for a more dramatic correction.
Less reliance on post-op compliance
Since results are achieved during surgery, families do not have to worry about helmet therapy adherence.
Downsides of CVR
The main downside of cranial vault remodeling is that it is a more invasive procedure, causing more swelling and requiring a longer hospital stay and recovery. However, for babies who are not eligible for endoscopic surgery due to age or case severity, it remains the gold standard for craniosynostosis correction.

Which Procedure is Best for Your Child?

The Baby’s Age
- Under 3 months – Endoscopic suturectomy is an option (if helmet therapy is feasible).
- Over 6 months – Cranial vault remodeling is likely the better choice.
The Severity of the Skull Deformity
- Mild to moderate craniosynostosis – Endoscopic suturectomy may work well.
- Severe skull distortion? Cranial vault remodeling offers a more immediate and controlled correction.
Parental Preference & Commitment to Helmet Therapy
- Families who are comfortable with long-term helmet therapy often prefer endoscopic surgery.
- Parents who want immediate results and minimal follow-up care may choose CVR.
Who will guide this decision?
- A craniofacial surgeon will help guide this decision, taking into account your child’s specific condition, your preferences, and the expected long-term results.

Parental Perspective: What Do Families Say About Their Experiences?
Parents who choose endoscopic suturectomy often appreciate the quick recovery, minimal scarring, and lower surgical risks, but they also emphasize the importance of commitment to helmet therapy. Some families initially express concerns about the helmet but later find that their baby adjusts quickly, and they are thrilled with the final results.
On the other hand, parents who choose cranial vault remodeling often feel relieved to have a one-time surgery with no follow-up helmet therapy. Many families appreciate seeing the immediate correction in their child’s head shape and feel reassured that no further interventions will be needed.
Both procedures have high success rates, and ultimately, most families feel confident in their choice once they see their child’s progress.
Complications and Challenges
Bleeding and Blood Loss
Endoscopic suturectomy is much less invasive than cranial vault remodeling, meaning blood loss is minimal and the need for a blood transfusion is rare. However, as with any surgery, there is still a small risk of bleeding, especially since the skull bones contain many tiny blood vessels.
To minimize this risk, surgeons use advanced techniques to control bleeding, including cauterization (sealing blood vessels during surgery) and bone wax (a specialized material that helps stop bleeding in bones). If bleeding occurs after surgery, it is usually minor and resolves on its own, but in extremely rare cases, a follow-up procedure may be necessary to address it.
Infection
Any time a surgical incision is made, there is a risk of infection, though this is very uncommon with endoscopic suturectomy.
The incisions are small and heal quickly, significantly reducing the chance of bacteria entering the surgical site.To further lower this risk:
- The surgical team follows strict sterile protocols during the procedure.
- Babies receive a short course of antibiotics before and sometimes after surgery.
- Parents are given detailed wound care instructions to keep the incision sites clean at home.
Signs of Infection
Signs of infection include:
- Redness, warmth, or swelling around the incisions
- Fever (above 100.4°F or 38°C)
- Pus or unusual drainage from the surgical site
- Irritability or excessive sleepiness
If any of these symptoms occur, you should contact your doctor immediately, as early treatment with antibiotics can quickly resolve the issue.
Dural Tears and Cerebrospinal Fluid Leaks
The dura is the thin, protective membrane that covers the brain. During surgery, the surgeon takes great care to avoid injuring the dura, but in rare cases, a small tear can occur. If this happens, cerebrospinal fluid (CSF) surrounding the brain may leak.
This complication is uncommon, and in most cases, small tears are repaired during surgery using a special sealant. If a CSF leak is noticed after surgery (e.g., fluid leaking from the incision), the surgeon may recommend a short hospital stay for observation or, in rare cases, a minor procedure to seal the leak.
Incomplete Skull Correction
Endoscopic suturectomy relies on natural skull growth and helmet therapy to achieve the desired results.
If helmet therapy is not followed correctly, the skull may not reshape as expected, leading to:- Residual head asymmetry
- Uneven skull expansion
- A need for additional procedures later in childhood
To prevent this, it’s essential to stay consistent with helmet use (23 hours per day) and attend all follow-up visits with the orthotist and surgeon. If the skull is not shaping properly, minor helmet adjustments can usually correct the issue before it becomes a long-term concern.
Challenges Parents May Face
Helmet Therapy Compliance
For many parents, adjusting to helmet therapy is one of the biggest challenges after surgery. Common concerns include:
- “Will my baby be uncomfortable?” – Most babies adjust within a few days and don’t seem to mind the helmet.
- “What if my baby gets hot?” – Helmets are lightweight and ventilated, but you should monitor your baby for overheating.
- “Will people stare or make comments?” – Some parents feel self-conscious about the helmet, but many find support through online communities of other families going through similar experiences.
The key to success is consistency—the more the helmet is worn, the better the results. Parents who stick to the schedule often see steady improvement in their child’s head shape within weeks.
Emotional Stress and Anxiety
It’s completely normal to feel overwhelmed, nervous, or even guilty about your child needing surgery. Some common emotions include:
- Worry about the procedure itself – Surgery, even minimally invasive, can be nerve-wracking for parents.
- Frustration with helmet therapy – Seeing slow, gradual improvements instead of immediate results can be challenging.
- Concerns about long-term outcomes – Parents often wonder if their child’s head will look completely normal in the future.
Support from doctors, other parents, and loved ones can make a big difference. Many parents find comfort in joining support groups or online forums where they can connect with others who have gone through the same experience.
Sleep and Comfort Adjustments
After surgery, some babies experience temporary sleep disturbances due to:
- Helmet adjustments – Some babies take a few nights to get used to sleeping with the helmet.
- Mild swelling – Swelling is usually minimal but can cause temporary discomfort.
- Changes in sleep position – Some babies need time to find a comfortable sleeping position with the helmet on.
These challenges typically resolve within a week or two, and most babies return to their normal sleep patterns quickly.
How To Ensure the Best Outcome
While complications are rare, there are simple steps parents can take to help ensure a smooth recovery:
- Follow all postsurgical care instructions – Keep the incisions clean and monitor them for signs of infection.
- Stay consistent with helmet therapy – Wearing it 23 hours per day is key to achieving the best results.
- Attend all follow-up appointments – Regular visits with the surgeon and orthotist ensure that everything is progressing as expected.
- Be patient with progress – The skull reshapes gradually, so noticeable improvement takes weeks to months.
- Ask for support when needed – Whether from doctors, other parents, or online communities, support can make the process easier.


Future Directions & Innovations in Craniosynostosis Treatment
Medical advancements are constantly improving the diagnosis and treatment of craniosynostosis. While endoscopic suturectomy has revolutionized early treatment, ongoing research and new technologies continue to push the field forward, aiming for even safer, more effective, and less invasive options.
From advancements in surgical techniques to improved helmet therapy designs and potential nonsurgical interventions, the future of craniosynostosis treatment looks promising. Parents considering treatment can feel confident that they are benefiting from cutting-edge medical care, and future generations may have even more refined options available.

Ultrasound as a Radiation-Free Diagnostic Tool
Early detection is critical for successful endoscopic suturectomy, but diagnosing craniosynostosis in very young infants can sometimes be challenging. New imaging techniques are making it easier to confirm the condition earlier and more accurately, allowing for timely intervention.
- While CT scans remain the gold standard for confirming craniosynostosis, they expose infants to a small amount of radiation.
- High-resolution ultrasound is emerging as a safer, radiation-free alternative that can detect suture fusion in very young infants, potentially leading to earlier diagnosis and treatment.
Artificial Intelligence and 3D Modeling for Diagnosis
- Researchers are developing AI-based tools that can analyze head shape measurements and predict craniosynostosis with high accuracy.
- 3D imaging software is becoming more sophisticated, enabling better visualization of skull deformities without the need for invasive scans.
Faster and more reliable diagnosis means more babies can be identified in time for minimally invasive treatments, avoiding the need for more complex surgeries later in life.
Improvements in Surgical Techniques
Even though endoscopic suturectomy is already a minimally invasive procedure, surgeons are exploring ways to make it even safer and more precise.
Robot-Assisted Surgery
- Robotic guidance systems are being tested to improve the precision of bone removal while reducing operative time.
- These systems allow surgeons to navigate delicate areas more accurately, potentially reducing the risk of complications such as dural tears or excessive bleeding.
Augmented Reality in the Operating Room
- Some hospitals are exploring the use of augmented-reality overlays during surgery, providing real-time, 3D visualizations of the skull and sutures.
- This allows for even greater precision in removing only the necessary portions of bone while minimizing impact on surrounding structures.
As these technologies become more widely available, endoscopic procedures may become even more effective, further reducing the risks and improving outcomes.
Innovations in Helmet Therapy
Helmet therapy has been a key part of postsurgical success, but new developments are making helmets lighter, smarter, and more effective.
3D-Printed Custom Helmets
- Traditional helmets are custom fitted but require manual adjustments as the baby grows.
- Newer 3D-printed helmets are being designed to adapt more precisely to each baby’s head, improving comfort and effectiveness.
Smart Helmets With Sensors
- Some researchers are developing helmets with embedded sensors that track head growth in real time.
- These devices can send alerts to parents and orthotists if adjustments are needed, ensuring the helmet is always guiding growth properly.
These advancements could make helmet therapy more convenient for parents and more effective for the child, potentially reducing the overall wear duration while achieving even better results.
Exploring Nonsurgical Treatment Possibilities
One of the most exciting areas of research is the potential for nonsurgical treatments that could prevent or reverse suture fusion without the need for surgery.
Biologic Therapies To Prevent Suture Fusion
- Scientists are investigating the use of molecular inhibitors that could block premature suture fusion, potentially allowing the skull to grow normally without surgery.
- Some studies suggest that gene therapy could one day be used to prevent craniosynostosis in at-risk infants.


Stem Cell and Bone Regeneration Research
- Research in bone regeneration may eventually lead to less invasive ways of correcting skull deformities.
- Future treatments could involve injectable stem cells or biologic scaffolds that promote healthy skull growth without the need for surgical intervention
While these treatments are still in early stages, they represent a hopeful future where craniosynostosis could be managed with even fewer interventions.Expanding Access to Specialized Care
Despite advancements in craniosynostosis treatment, access to specialized craniofacial centers is still a challenge for some families. New initiatives are working to improve the availability and affordability of care.
Telemedicine and Remote Consultations
- Virtual consultations allow families in rural or underserved areas to connect with leading craniofacial specialists without extensive travel.
- This ensures faster diagnosis and treatment planning, helping more babies access early care.
Insurance and Cost Advocacy
- Efforts are underway to increase insurance coverage for helmet therapy and craniosynostosis surgeries, reducing financial barriers for families.
- Some organizations are working to expand financial assistance programs for families who need support covering treatment costs.
By improving access to expert care, more children can receive timely, effective treatment, regardless of where they live.
Key Takeaways
Craniosynostosis is treatable
With early intervention, either through endoscopic suturectomy or cranial vault remodeling, most children achieve excellent outcomes, with normal skull growth and development.
Timing matters
Endoscopic suturectomy is most effective before 3 months of age, while cranial vault remodeling is better suited for infants 6-12 months old or those with more severe skull deformities.
Helmet Therapy is essential for endoscopic surgery
Helmet therapy is essential for endoscopic surgery. The success of endoscopic suturectomy depends on consistent helmet wear (23 hours per day for 6-12 months) to guide proper skull growth.
Choosing Endoscopic Suturectomy or Cranial Vault Remodeling
Whether choosing endoscopic suturectomy or cranial vault remodeling, both procedures have excellent long-term results with minimal risk of complications when performed by an experienced craniofacial team.
There are minimal long-term effects
There are minimal long-term effects. Once treated, most children experience normal brain development, engage in physical activity, and lead their daily lives with no restrictions or ongoing medical concerns.
Support is available
Parents don’t have to navigate this journey alone—there are craniosynostosis support groups, online communities, and medical professionals who can help every step of the way.
Actionable Steps for Parents
If You Suspect Your Baby Has Craniosynostosis
Observe your baby’s head shape and symmetry—does it seem unusually elongated, flattened, or misshapen?
- Bring up concerns with your pediatrician as soon as possible.
- Request a referral to a craniofacial specialist for further evaluation.
- If needed, ask about imaging tests (CT scan or ultrasound) to confirm the diagnosis.
If Your Child Has Been Diagnosed
- Discuss treatment options with a craniofacial surgeon and ask if your baby qualifies for endoscopic suturectomy.
- If your baby is under 3 months old, schedule surgery as soon as possible to keep endoscopic options open.
- If your baby is older than 6 months, consult with your doctor about cranial vault remodeling and its benefits.
- Ask detailed questions about surgical risks, recovery, and expected outcomes.
If Your Child is Undergoing Endoscopic Suturectomy
- Schedule a helmet therapy consultation before surgery so you’re prepared for the post-op phase.
- Plan for helmet fitting within one to two weeks after surgery to ensure proper skull growth guidance.
- Stay committed to helmet wear (23 hours per day) and attend regular adjustments with the cranial orthotist.
- Keep up with follow-up visits with the surgeon to track skull growth and progress.
If Your Child is Undergoing Cranial Vault Remodeling
- Prepare for a longer hospital stay (three to five days) and initial swelling, which is normal.
- Follow post-op care instructions to keep incisions clean and monitor them for signs of infection.
- Attend routine follow-ups with the surgeon to ensure proper skull healing.
- No helmet therapy is required—your child’s skull reshaping is complete after surgery.
If Your Child Has Completed Treatment
- Celebrate the end of the journey—most children require no further intervention.
- If your child has small scars, apply gentle scar creams or massage techniques as recommended by your doctor.
- Monitor head growth during routine pediatric visits to ensure everything continues developing normally.
- If any concerns arise later, reach out to your craniofacial specialist for guidance.