Fronto-Orbital Advancement for the Treatment of Craniosynostosis
A Guide for Parents
Craniosynostosis is a condition that can be overwhelming for any parent to face. The idea that your child’s skull is not growing as it should, potentially affecting brain development and facial appearance, is understandably concerning. But thanks to advances in craniofacial surgery, effective treatment options are available. One of the most widely used and successful surgical interventions is fronto-orbital advancement (FOA), a procedure designed to reshape the skull and forehead, providing the space necessary for proper brain growth.
This section is written specifically for parents who are navigating the FOA journey for their child. We understand that the amount of medical information available can be overwhelming, filled with complex terminology and difficult decisions. Our goal is to provide a clear guide that explains what FOA is, how it works, and what you can expect throughout the process.
Fronto-Orbital Advancement for the Treatment of Craniosynostosis
A Guide for Parents

Table Of Contents

What Is Fronto-Orbital Advancement (FOA)?
FOA is a surgical procedure designed to correct frontal craniosynostosis, a condition where the sutures in the front of the skull fuse too early. This can lead to abnormal skull and forehead shape, increased intracranial pressure (ICP), and potential developmental concerns.
FOA aims to restore normal skull growth by surgically removing, reshaping, and repositioning the forehead and upper eye sockets (orbits) to create a more natural skull contour and allow for healthy brain development.
There are two main approaches to FOA:
- Traditional open FOA: This more invasive technique involves a large incision and direct reshaping of the skull bones. It has been the standard treatment for many years and is often used for older infants and severe cases.
- Endoscopic FOA: This minimally invasive alternative uses smaller incisions and relies on helmet therapy after surgery to gradually guide skull growth. It is typically only an option for younger infants, usually under 4-6 months of age.
Each of these approaches has its benefits, risks, and recovery processes, all of which will be discussed in detail throughout this section.
Why Fronto-Orbital Advancement? Understanding the Need for Surgery
The primary goal of FOA is not only to provide cosmetic correction but also to ensure proper brain growth and function. When the skull’s natural growth is restricted due to early suture fusion, it can sometimes lead to increased ICP, developmental delays, and long-term complications. FOA helps prevent these issues by creating the space necessary for normal brain development.
Additionally, FOA plays a role in restoring a natural appearance to the forehead and upper facial region. Many parents worry about the long-term psychosocial impact of an abnormal head shape, and FOA provides an effective solution for improving both function and appearance.


Diagnosis
One of the first and most important steps in your child’s journey with craniosynostosis is obtaining an accurate diagnosis. For many parents, the first sign that something may be different about their child’s skull shape comes either at birth or within the first few months of life. While some irregularities in head shape are common and resolve on their own, others may indicate an underlying condition such as craniosynostosis.
In this section, we will break down the process of diagnosing craniosynostosis, including the signs parents may notice, how doctors evaluate the condition, and the tests used to confirm the need for treatment.
Recognizing the Signs of Craniosynostosis
Craniosynostosis occurs when one or more of the cranial sutures (the soft, flexible joints between the bones of a baby’s skull) close too early. These sutures normally remain open during early childhood to allow for brain growth and skull expansion. When one of them fuses prematurely, it restricts normal growth patterns, leading to an irregular head shape.
With craniosynostosis involving the frontal and orbital bones—the type most commonly treated with FOA—you or your child’s pediatrician may notice:
- A misshapen forehead: One side may appear flattened, while the opposite side bulges forward (in cases of unicoronal craniosynostosis).
- Orbital asymmetry: One eye may appear higher than the other, or the shape of the eye socket may look different.
- A ridge along the fused suture: Sometimes, a noticeable bony ridge can be felt where the suture has closed too early.
- Lack of a “soft spot” (fontanelle) or a very small one: The anterior fontanelle may be absent or feel unusually firm.
- Skull asymmetry that does not improve over time: Unlike positional plagiocephaly (caused by external pressure on the skull), craniosynostosis does not improve with repositioning.
When To Seek a Medical Evaluation
While some minor skull shape irregularities can be normal in newborns, persistent or worsening asymmetry should prompt a visit to your child’s pediatrician. The earlier craniosynostosis is diagnosed, the more treatment options may be available.
For example, endoscopic FOA is typically only an option for infants under 3 months old, making early diagnosis critical.
If the pediatrician suspects craniosynostosis, they will refer your child to a craniofacial specialist or pediatric neurosurgeon for further evaluation.
How Doctors Diagnose Craniosynostosis
A diagnosis of craniosynostosis is typically made through a combination of physical examination and imaging studies.
Physical examination
A trained specialist will assess your baby’s head shape by:
- Feeling for suture ridges or missing soft spots
- Checking for forehead or orbital asymmetry
- Measuring head circumference to assess growth over time
- Evaluating facial symmetry and how the skull appears from different angles
A thorough physical exam provides important clues, but imaging is often necessary to confirm the diagnosis and guide treatment planning.
Imaging studies
If craniosynostosis is suspected, doctors will typically order imaging to get a clearer picture of the skull structure. Several imaging options exist:
- 3D CT scan: This is the gold standard for diagnosing craniosynostosis. A 3D CT scan provides a detailed view of the skull bones and sutures, allowing doctors to see which sutures are fused and how the skull is being affected.
- X-rays: While their use is less common, X-rays can help identify suture closure in some cases.
- MRI: Occasionally, MRIs are used to evaluate brain development and ICP, but they are not typically needed for diagnosis alone.
Once imaging is completed, the craniofacial team will confirm the diagnosis and determine whether FOA is the best treatment option for your child.
Differentiating Craniosynostosis From Other Skull Shape Abnormalities
Not every irregular head shape is caused by craniosynostosis. Some infants develop positional plagiocephaly, a condition in which the skull becomes misshapen due to external pressure (such as lying in the same position for extended periods).
Unlike craniosynostosis, positional plagiocephaly does not involve premature suture fusion and can often be corrected with repositioning techniques or helmet therapy.

Key differences between craniosynostosis and positional plagiocephaly
| Feature | Craniosynostosis | Positional Plagiocephaly |
|---|---|---|
| Cause | Premature fusion of skull sutures | External pressure on the skull |
| Head shape | More rigid and asymmetrical | May improve with repositioning |
| Suture ridge | Often present | Not present |
| Soft spot (fontanelle) | May be missing or abnormally small | Usually open and normal |
| Treatment | Often requires surgery (FOA) | Often managed with repositioning or helmet therapy |
Cause
- Craniosynostosis
Premature fusion of skull sutures - Positional Plagiocephaly
External pressure on the skull
- Craniosynostosis
Head shape
- Craniosynostosis
More rigid and asymmetrical - Positional Plagiocephaly
May improve with repositioning
- Craniosynostosis
Suture ridge
- Craniosynostosis
Often present - Positional Plagiocephaly
Not present
- Craniosynostosis
Soft spot (fontanelle)
- Craniosynostosis
May be missing or abnormally small - Positional Plagiocephaly
Usually open and normal
- Craniosynostosis
Treatment
- Craniosynostosis
Often requires surgery (FOA) - Positional Plagiocephaly
Often managed with repositioning or helmet therapy
- Craniosynostosis
Indications and Patient Selection
FOA is primarily indicated for craniosynostosis involving the forehead and upper eye sockets, particularly coronal and metopic craniosynostosis. However, choosing between traditional open FOA and endoscopic FOA depends on factors such as age, severity, and suture involvement.
In this section, we will explore the criteria for selecting FOA as a treatment option, including when it is necessary, which children are eligible for surgery, and how surgeons decide between the open and endoscopic approaches.

When Is Fronto-Orbital Advancement Needed?

FOA is typically recommended in cases where premature fusion of the metopic suture or coronal suture(s) leads to:
- Severe skull asymmetry affecting the forehead and eye sockets
- Orbital asymmetry, which may cause one eye to appear higher than the other
- Restrictive skull growth that could lead to increased ICP (this is less common in single-suture cases)
- Psychosocial concerns regarding appearance and potential social impact as the child grows
Because cranial sutures exist to allow brain growth, their premature closure can lead to compensatory skull deformities as other areas of the head grow abnormally to accommodate the brain. If left untreated, the resulting skull deformities can be difficult to correct later in life.
What Types of Craniosynostosis Require FOA
- Unicoronal
- Bicoronal
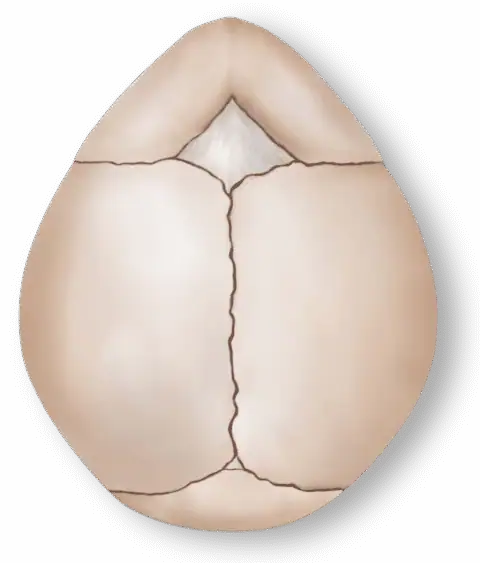
- Metopic
Metopic
- Overview
- Suture involved: One coronal suture (either left or right) is affected.
- Head shape: The forehead is asymmetrical, with one side flattened and the opposite side excessively prominent.
- Orbital asymmetry: One eye may appear higher or have a different shape than the other.
- Why FOA? The procedure corrects the forehead and orbital asymmetry, improving both cosmetic and functional outcomes.

The overall incidence of Craniosynostosis is approximately 1 in 2000/3000 births. Metopic synostosis is relatively rare, accounting for between 5% and 15% of all craniosynostosis cases.
Diagnostically, the condition can be identified through a physical examination, where the triangular shape of the forehead and ridging are noticeable. Imaging techniques, such as computed tomography (CT) scans, can confirm the diagnosis and assess the extent of the fusion.
Treatment typically involves surgery to correct the skull shape and allow for normal brain growth. The surgical procedure, usually performed in the first year of life, involves removing and reshaping the fused bones to create a more typical skull contour. Please refer to our Treatment Options page for a more detailed explanation of these surgical procedures.
Coronal
- Overview
- Sutures involved: Both coronal sutures are affected.
- Head shape: The skull is shortened from front to back, with a tall, wide forehead (known as brachycephaly).
- Why FOA? FOA reshapes the forehead and orbits, allowing for more proportional skull growth.
The overall incidence of Craniosynostosis is approximately 1 in 2000/3000 births. Coronal synostosis accounts for approximately 20% to 30% of all craniosynostosis cases.
Diagnosis of coronal synostosis involves a thorough physical examination where asymmetry or brachycephaly is apparent. Imaging techniques, including CT scans, help confirm the diagnosis and plan the surgical intervention.
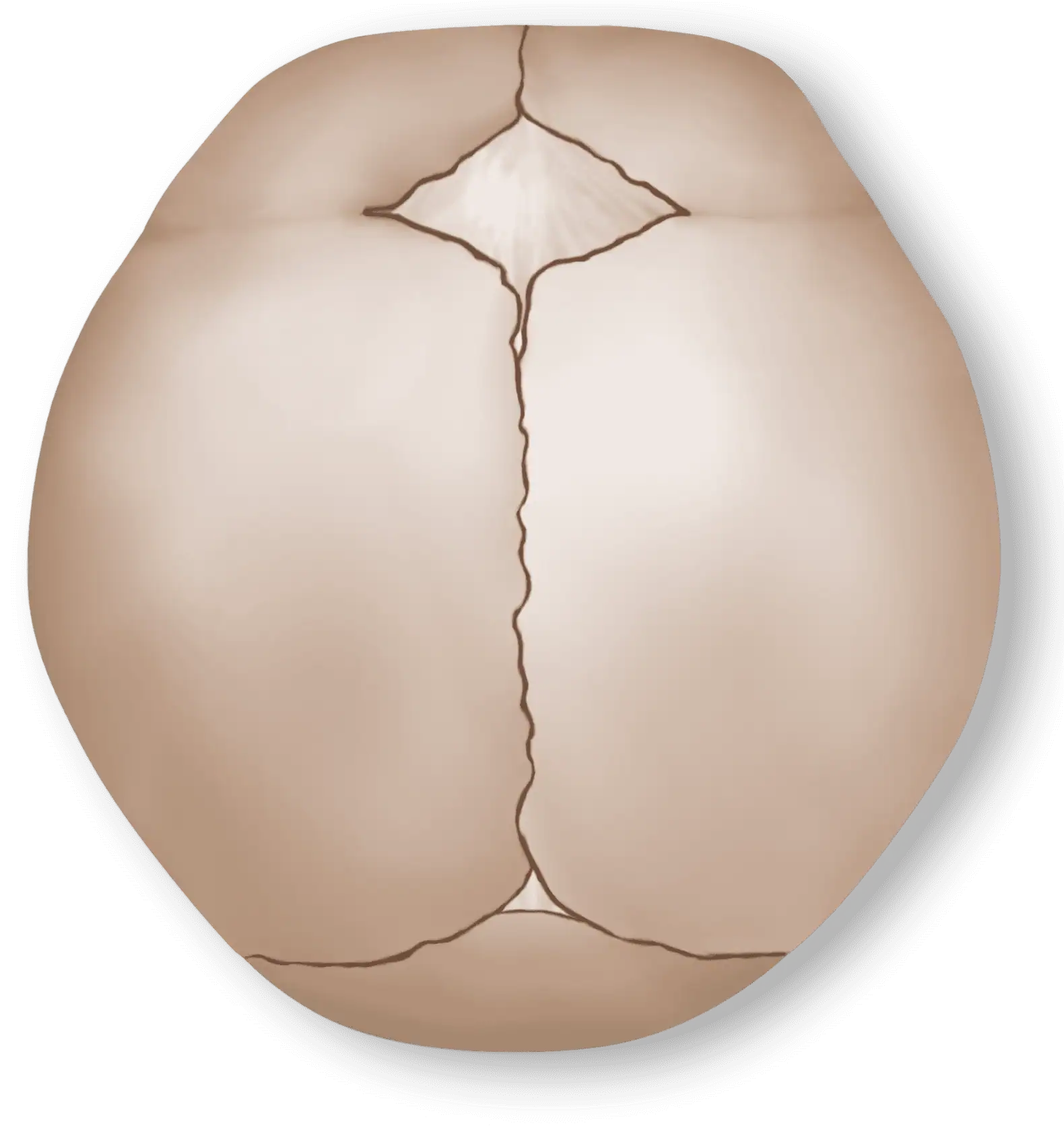
Sagittal
- Overview
- Suture involved: The metopic suture (the suture running down the middle of the forehead) is affected.
- Head shape:The forehead is triangular, with a ridge running down the middle.
- Why FOA? The procedure helps to widen the forehead and restore a more natural contour.
FOA is not typically used for other forms of craniosynostosis, such as sagittal or lambdoid synostosis, which require different surgical techniques.
The overall incidence of Craniosynostosis is approximately 1 in 2000/3000 births. Sagittal synostosis accounts for approximately 40% to 55% of all craniosynostosis cases.
Physical examination often reveals a long, narrow head shape with a prominent ridge along the sagittal suture. Confirmatory diagnosis is achieved through imaging studies such as CT scans, which provide detailed views of the fused suture and skull shape.
Surgical treatment for sagittal synostosis aims to expand the width of the skull and improve its overall shape. Depending on the severity of the condition, procedures may include minimally invasive endoscopic suturectomy or a more complex procedure referred to as cranial vault remodeling. Please refer to our Treatment Options page for a more detailed explanation of these surgical procedures.
Choosing Between Open and Endoscopic Fronto-Orbital Advancement
Once your child is identified as needing FOA, the next critical decision is whether they are eligible for endoscopic FOA or if they require traditional open FOA.
The main deciding factor is age at the time of diagnosis.
| Feature | Traditional open FOA | Endoscopic FOA |
|---|---|---|
| Age | Typically performed between 6-12 months | Best suited for infants under 3 months |
| Invasiveness | More invasive; requires a larger incision and direct reshaping of bone | Less invasive; smaller incisions and bone removal without reshaping |
| Helmet therapy required? | No, bone is reshaped during surgery | Yes, helmet therapy guides skull growth post-surgery |
| Hospital stay | Longer (three to five days) | Shorter (one or two days) |
| Recovery time | Longer recovery due to extensive bone work | Faster recovery, with less blood loss and swelling |
| Best for | Older infants with severe skull deformities or when endoscopic FOA is no longer an option | Younger infants diagnosed early with mild to moderate deformities |
Age Requirement
- Endoscopic Suturectomy
Performed before 3 months of age - Cranial Vault Remodeling (CVR)
Performed between 6–12 months
- Endoscopic Suturectomy
Surgical Approach
- Endoscopic Suturectomy
Minimally invasive (small incisions) - Cranial Vault Remodeling (CVR)
Open surgery (large incision across the scalp)
- Endoscopic Suturectomy
Procedure Time
- Endoscopic Suturectomy
About 1 hour - Cranial Vault Remodeling (CVR)
3–5 hours
- Endoscopic Suturectomy
Blood Loss
- Endoscopic Suturectomy
Minimal, low chance of transfusion - Cranial Vault Remodeling (CVR)
Higher blood loss, higher chance of transfusion.
- Endoscopic Suturectomy
Hospital Stay
- Endoscopic Suturectomy
1 day or overnight - Cranial Vault Remodeling (CVR)
3–5 days
- Endoscopic Suturectomy
Recovery Time
- Endoscopic Suturectomy
Faster, minimal swelling - Cranial Vault Remodeling (CVR)
Longer, significant swelling
- Endoscopic Suturectomy
Helmet Therapy
- Endoscopic Suturectomy
Required for 6–12 months - Cranial Vault Remodeling (CVR)
Not required
- Endoscopic Suturectomy
Results Timeline
- Endoscopic Suturectomy
Gradual improvement over time - Cranial Vault Remodeling (CVR)
Immediate reshaping
- Endoscopic Suturectomy
Ideal case severity
- Endoscopic Suturectomy
Mild to moderate cases - Cranial Vault Remodeling (CVR)
Moderate to severe cases
- Endoscopic Suturectomy
Long-Term Outcomes
- Endoscopic Suturectomy
Excellent if helmet therapy is followed - Cranial Vault Remodeling (CVR)
Excellent, no helmet needed
- Endoscopic Suturectomy

Patient Age: A Key Factor in Fronto-Orbital Advancement Selection
Endoscopic FOA is only an option for infants diagnosed early, typically before 3 months of age. This is because helmet therapy is essential for guiding skull growth, and older infants no longer have the same skull flexibility to achieve correction through helmeting alone.
If your child is older than 6 months at the time of diagnosis, open FOA is usually the only option.
Other Considerations for Surgery Selection
While age is the most important factor in determining whether open or endoscopic FOA is appropriate, other factors may influence the decision, including:
- Severity of the skull deformity: More severe cases may require open FOA for more precise reshaping.
- Presence of increased ICP: If ICP is detected, open FOA is preferred as it allows for more extensive skull expansion.
- Syndromic versus nonsyndromic craniosynostosis: Children with syndromic craniosynostosis (e.g., Apert, Crouzon, or Pfeiffer syndrome) may require a more complex open FOA procedure.
What if Surgery Is Delayed?
For some families, surgery may be delayed due to late diagnosis, medical concerns, or family decisions. If FOA is postponed beyond the ideal treatment window, additional surgical modifications or alternative procedures may be required.
In older children, distraction osteogenesis (a technique where bones are gradually expanded) may be needed instead of FOA.
Making the Best Decision for Your Child
Choosing the right surgical approach can feel overwhelming, but your craniofacial surgeon and neurosurgeon will guide you through the decision-making process based on:
- Your child’s age at diagnosis
- Severity of the skull deformity
- Risk factors, such as increased ICP
- Family preferences and discussions on treatment goals
Preoperative Preparation
Once the decision has been made for your child to undergo FOA, the next step is preparing for surgery. This phase can feel overwhelming for parents, as it involves medical evaluations, consultations, and logistical planning. Understanding what to expect in the days and weeks leading up to surgery can help you feel more confident and prepared.
In this section, we will cover the essential steps in preoperative preparation, including medical tests, consultations with specialists, what to expect on the day of surgery, and how to emotionally prepare your child and family.

Medical Evaluations Before Surgery
Evaluations
Before undergoing FOA, your child will need a series of preoperative evaluations to ensure they are healthy enough for surgery and to allow the surgical team to plan the procedure.
Imaging studies
Although the diagnosis of craniosynostosis has already been made, additional imaging may be required to help the surgical team plan the procedure. This may include:
- 3D CT scan: The scan provides a detailed view of the skull structure, bone thickness, and exact areas of abnormal fusion.
- MRI: In some cases, an MRI may be performed to evaluate ICP or brain development.
Blood tests and lab work
Routine bloodwork is required to ensure that your child is healthy for surgery.
These tests may include:
- Complete blood count: This is done to check for anemia, infection, or other blood-related issues.
- Blood typing and crossmatching: Since FOA can involve some blood loss, this ensures that compatible blood is available if needed.
- Coagulation tests (PT, PTT, INR): These tests assess blood clotting ability to minimize bleeding risks during surgery.
Cardiac and respiratory evaluation
If your child has any underlying medical conditions, additional assessments may be necessary, including:
- Echocardiogram: For children with suspected or diagnosed syndromic craniosynostosis, a heart evaluation may be required.
- Pulmonary function tests: If your child has breathing difficulties, a pulmonologist may be consulted before surgery.

Logistics and Preparing for Your Hospital Stay

What To Pack for Surgery Day
For your child:
-
Comfortable clothing (zip-up onesies or button-down shirts)
-
A favorite blanket or stuffed animal for comfort
-
Extra diapers and wipes
-
Formula or breastmilk if needed for after surgery
For you:
-
ID and insurance cards
-
Comfortable clothes and toiletries for your overnight stay
-
Snacks and water
-
Phone charger
-
A notepad to write down important information from doctors
-
Hospital Stay Expectations
- Endoscopic FOA usually requires a one- or two-day hospital stay.
- Traditional open FOA requires a three- to five-day hospital stay due to longer recovery time and monitoring for swelling.
Most children are admitted the morning of surgery, and the first 24-48 hours of their stay are the most intense due to swelling and postanesthesia effects.
Surgery Day: What To Expect
On the morning of surgery:
- Check-in at the hospital: You will complete the final paperwork and preoperative assessments.
- Anesthesia consultation: The anesthesiologist will review the sedation plans and ensure your child is safe for general anesthesia.
- Preoperative preparation: Your child will be changed into a hospital gown, and vital signs will be taken.
- Parental goodbyes: Parents are typically allowed to stay with their child right up until the child is taken into the operating room.
After your child is taken through to surgery, you will be guided to a waiting area. The surgical team will provide updates throughout the procedure.
Final Thoughts on Preparing for Fronto-Orbital Advancement
The days leading up to FOA can be filled with many emotions—anticipation, anxiety, and hope.
Being well informed and prepared will not only help you feel more in control but will also allow you to focus on providing the best possible support for your child.
The Procedure
FOA is a complex but well-established surgical procedure designed to reshape the forehead and upper eye sockets (orbits) in children with craniosynostosis. The goal is to correct abnormal skull growth caused by premature suture fusion, allowing for normal brain expansion and improving the child’s facial symmetry.
The procedure can be performed using two main approaches:
- Traditional open FOA: A more invasive technique involving direct reshaping of the skull
- Endoscopic FOA: A minimally invasive alternative for younger infants that requires postoperative helmet therapy
In this section, we will provide a detailed, step-by-step breakdown of both surgical techniques, including what happens in the operating room, how the bones are reshaped, and what you can expect during and immediately after surgery.

Traditional Open Fronto-Orbital Advancement: An Overview

Traditional open FOA is the most commonly performed technique for treating craniosynostosis affecting the forehead and orbits. It involves making an incision across the scalp, removing and reshaping the affected skull bones, and securing them in a new position using plates, sutures, or bioresorbable materials.
This approach is preferred for:
- Older infants (typically 6 months or older)
- More severe skull deformities
- Cases with increased ICP
- Syndromic craniosynostosis requiring extensive reshaping
Step-By-Step Breakdown of Open FOA
1.
Anesthesia
- The child is placed under general anesthesia to ensure they remain asleep and pain-free throughout surgery.
- The child’s head is carefully positioned and stabilized using a padded headrest or a specialized cranial fixation device to prevent movement.
2.
Incisions
- An incision is made across the scalp, from ear to ear (coronal incision). It is made in a way to help reduce visible scarring and allow hair to grow over the scar.
- The skin, underlying tissue, and periosteum (protective layer covering the skull) are carefully lifted to expose the frontal bone and orbital rims.
3.
Bone reshaping
- The surgeon carefully removes the affected section of the forehead and orbital bones, making precise cuts to separate fused sutures and allow for reshaping.
- The frontal bone (forehead) is reshaped to create a more natural contour, correcting any asymmetry.
- If needed, the upper eye socket (orbital bandeau) is also reshaped to ensure proper alignment and prevent orbital dystopia (uneven eye height).
4.
securing the bones
- The newly shaped bone segments are secured in place using:
— Absorbable plates and screws: Biodegradable materials dissolve over time as the skull heals.
— Suture fixation: In younger infants, strong sutures may be used instead of plates.
— Bone grafts (if needed): Small bone grafts may be placed to fill gaps and ensure stability.
5.
Closure
- The scalp is repositioned, and the incision is closed using absorbable sutures or skin glue.
- A light compression bandage is applied to help minimize swelling.
6.
Duration
- Open FOA typically takes three to five hours to complete.
- Blood loss is moderate, and some infants may require a blood transfusion during or after surgery.

Advantages and Considerations of
Open Fronto-Orbital Advancement
- Highly effective for moderate to severe cases
- Provides immediate skull reshaping
- No need for postoperative helmet therapy
- Longer recovery time
- Higher risk of swelling and blood loss
- More invasive with a longer hospital stay (three to five days)
Endoscopic Fronto-Orbital Advancement: An Overview
Endoscopic FOA is a minimally invasive alternative that involves making small incisions and using a tiny camera (endoscope) to assist in removing the fused suture. Unlike open FOA, no extensive reshaping is done during surgery; instead, the skull is allowed to reshape gradually with helmet therapy after surgery.
This approach is only an option for younger infants, typically:
- Under 3 months old
- With mild to moderate cranial deformities
- Diagnosed early enough for helmet therapy to be effective

Step-By-Step Breakdown of Endoscopic Fronto-Orbital Advancement
1.
Anesthesia
- The child is placed under general anesthesia and positioned securely.
2.
incisions & endoscope
- Instead of a large scalp incision, two small incisions (about one to two centimeters each) are made on the scalp.
- A tiny camera (endoscope) is inserted to provide a magnified view of the skull sutures.
3.
Bone removal
- Using specialized surgical instruments, the fused suture is carefully removed to allow the skull to expand naturally.
- No direct bone reshaping is done; the helmet therapy will guide skull growth postoperatively.
4.
Closure
- The incisions are closed with dissolvable sutures, and a light dressing is applied.
5.
Duration
- Endoscopic FOA is much shorter, typically lasting one to two hours.
- There is minimal blood loss compared with open FOA, reducing the need for transfusions.
6.
Helmet Therapy
- Within one week after surgery, the infant is fitted for a custom-molded helmet that will gently shape the skull as it grows.

Advantages and Considerations of Endoscopic FOA
- Minimally invasive with smaller incisions
- Less swelling, pain, and blood loss
- Shorter hospital stay (one to two days)
- Requires strict helmet therapy for 6-12 months
- Only an option for younger infants (under 6 months)
- Less effective for severe cases
Choosing the Right Approach for Your Child
| Factor | Traditional Open FOA | Endoscopic FOA |
|---|---|---|
| Age requirement | Six months or older | Under 3 months |
| Invasiveness | More invasive (larger incision) | Minimally invasive (small incisions) |
| Bone reshaping | Completed during surgery; immediate | Guided over time with helmet therapy |
| Hospital stay | Three to five days | One to two days |
| Recovery time | Longer (weeks) | Shorter (days) |
| Helmet therapy? | No | Yes (6-12 months) |
Age requirement
- Traditional Open FOA
Six months or older - Endoscopic FOA
Under 3 months
- Traditional Open FOA
Invasiveness
- Traditional Open FOA
More invasive (larger incision) - Endoscopic FOA
Minimally invasive (small incisions)
- Traditional Open FOA
Bone reshaping
- Traditional Open FOA
Completed during surgery; immediate - Endoscopic FOA
Guided over time with helmet therapy
- Traditional Open FOA
Hospital stay
- Traditional Open FOA
Three to five days - Endoscopic FOA
One to two days
- Traditional Open FOA
Recovery time
- Traditional Open FOA
Longer (weeks) - Endoscopic FOA
Shorter (days)
- Traditional Open FOA
Helmet therapy?
- Traditional Open FOA
No - Endoscopic FOA
Yes (6-12 months)
- Traditional Open FOA

Postoperative Course
The period after FOA is a crucial time for recovery and healing. Parents often have many questions about what to expect in terms of hospital stay, pain management, swelling, and long-term healing. While the immediate postoperative period can feel overwhelming, understanding the recovery timeline can help you prepare and support your child.
This section will break down the postoperative course for both traditional open FOA and endoscopic FOA, including hospital care, at-home recovery, signs of complications, and long-term healing expectations.
Hospital Recovery: The First Few Days
Immediately after surgery
- Once surgery is complete, your child will be transferred to the postanesthesia care unit or monitoring as they wake up from anesthesia.
- Most infants will have an IV for fluids and pain medications, and in some cases, a small drain may be put in place to prevent fluid buildup under the scalp.
- Expect your child to be groggy, fussy, and possibly disoriented as the anesthesia wears off.
Swelling and bruising
- Swelling peaks around 24-48 hours after surgery and is most noticeable around the eyes and forehead.
- Some infants may experience temporary eye swelling that can shut their eyes completely, which can be alarming but is normal.
- Bruising is common around the eyes and cheeks and typically resolves within one to two weeks.
Pain management
- Pain is usually well controlled with a combination of:
— IV pain medications immediately after surgery
— Oral acetaminophen (Tylenol) or ibuprofen (Advil) once pain is manageable
— Morphine or stronger medications only if necessary
- Pain is usually well controlled with a combination of:
Hospital stay duration
- Traditional open FOA: Three to five days, depending on swelling, pain control, and overall recovery
- Endoscopic FOA: One or two days, since swelling and pain are significantly less
Most children are discharged once they are:
- Eating and drinking normally
- No longer needing IV pain medications
- Able to be comfortably managed at home

At-Home Recovery: The First Few Weeks

Traditional Open Fronto-Orbital Advancement: Home Care Instructions
Managing swelling and bruising:
- Swelling will gradually decrease over one to two weeks but may take longer to fully resolve.
- Keeping your child’s head elevated (using a semi-upright sleeping position) can help reduce swelling.
- A cold compress (wrapped in a soft cloth) can be gently applied to the forehead to ease discomfort.
Activity restrictions:
- Avoid strenuous activities or rough play for at least six to eight weeks.
- Supervise your child closely to prevent falls or head bumps.
- No tummy time for younger infants until cleared by the surgeon.
Incision care:
- Stitches are usually absorbable and do not need to be removed.
- Keep the incision clean and dry—only sponge baths are allowed until cleared for full bathing.
- Avoid scratching or rubbing the incision, especially as it heals and becomes itchy.
Endoscopic Fronto-Orbital Advancement: Home Care Instructions
Since Endoscopic FOA is minimally invasive, recovery is much quicker, but it requires strict helmet therapy afterward.
Helmet therapy:
- Helmet therapy begins within one week after surgery and continues for 6–12 months.
- The helmet guides skull growth to ensure proper reshaping.
- Regular helmet adjustments are needed every two to four weeks by a specialist.
General recovery guidelines:
- Swelling and discomfort are mild compared with open FOA.
- Activity restrictions are less stringent, but head protection is crucial since the skull is still reshaping.
Signs of Complications: When To Call the Doctor
While most children recover without issues, you should monitor for any signs of complications, including:
- Fever above 101°F (38.5°C), which could indicate infection
- Excessive redness, swelling, or pus from the incision, as these are signs of wound infection
- Persistent vomiting or refusal to eat, which may indicate pain or other issues
- Changes in alertness, unusual sleepiness, or difficulty waking, as these may be signs of increased ICP
- Bulging or sunken soft spot (fontanelle), which may indicate fluid buildup or dehydration
If any of these occur, contact your surgeon immediately.
Long-Term Healing and Follow-Up Appointments
Continued care and monitoring of your child’s progress is critical to ensure the best possible long-term results.
Follow-up schedule:
Your child will have regular follow-up visits to monitor healing and skull growth:
- One to two weeks after surgery: First post-op visit to check incision healing
- One month post-op: Assessment of skull shape and overall recovery
- Every three to six months for the first year: Continued monitoring of skull growth
For children who have undergone endoscopic FOA, helmet therapy adjustments are done every few weeks.
Scarring and hair growth:
- The incision scar fades over time and is usually hidden under the hair.
- Hair typically regrows within a few months, completely covering the surgical area.
Skull growth and long-term outcomes:
- The reshaped skull continues to develop naturally as the child grows.
- Additional surgeries are rare, but follow-up monitoring is important.
Outcomes and Long-Term Results
After undergoing FOA, parents naturally wonder: What will my child’s head look like in the long run? Will they need additional procedures? How does skull growth continue after surgery?
The good news is that FOA has excellent long-term success rates, with most children achieving normal skull shape, brain growth, and facial symmetry after surgery. However, recovery and results vary depending on the severity of the original deformity, the type of FOA performed (open vs. endoscopic), and individual healing factors.
This section will cover:
- Expected outcomes of FOA (cosmetic and functional improvements)
- How skull growth progresses over time
- Potential long-term issues and the rare need for additional procedures
- Psychosocial effects and self-esteem considerations as children grow

Cosmetic and Functional Outcomes
The improvement to your child’s head shape may be immediate or gradual, depending on the type or FOA. This section outlines what you can expect to see in the months following surgery.
Traditional Open Fronto-Orbital Advancement: Expected Results
- Immediate improvement in forehead and orbital shape: The forehead is reshaped during surgery, and parents will notice the results right away.
- Balanced facial symmetry: The previously flattened or protruding areas are corrected.
- Long-lasting correction: The newly reshaped forehead continues to grow with the child, maintaining normal proportions.
Mild irregularities may still be present, but in most cases, they are subtle and not noticeable to the average person.
Endoscopic Fronto-Orbital Advancement: Expected Results
- Gradual improvement over months: Since helmet therapy guides skull growth, changes are seen over time rather than immediately.
- Less dramatic reshaping compared with open FOA: While effective, results depend on helmet compliance and the child’s natural skull growth.
With consistent helmet use, the final head shape is often just as aesthetically pleasing as with open FOA, but it may take up to a year to see the full results.
Long-Term Skull Growth After Fronto-Orbital Advancement
One of the biggest concerns parents have is whether their child’s skull will continue growing normally after FOA. Fortunately, the answer is yes—FOA creates space for brain growth, allowing the skull to expand naturally over time:
- In most cases, no further surgery is needed once FOA has been performed.
- The reshaped bones fuse in their new position, and the skull grows proportionally as the child develops.
- Minor irregularities may self-correct over time as the skull continues to expand.
However, long-term monitoring is still important to ensure proper skull development.
Potential Long-Term Concerns
Although FOA is highly successful, a small percentage of children may require additional interventions for various reasons, including:
Residual skull irregularities:
- Some children may develop minor asymmetries as they grow, especially in severe preoperative cases.
- These irregularities are usually mild and do not require further surgery, but in rare cases, a revision surgery may be considered for cosmetic improvement.
Recurrent craniosynostosis (rare cases):
- In very rare cases, re-fusion of skull bones (resynostosis) can occur.
- If this happens, additional surgical interventions may be needed to prevent increased ICP or skull shape abnormalities.
The need for later orthognathic or facial surgery:
- Children with syndromic craniosynostosis (e.g., Apert, Crouzon syndrome) may require future jaw or facial surgeries as part of their ongoing care.
Psychological and Social Impact of Fronto-Orbital Advancement
As your child grows, self-image and confidence become important. You may be worried about how your child’s appearance will affect their social interactions, self-esteem, and overall well-being. FOA can help your child navigate this part of their live with more confidence.
Positive Psychological Outcomes
- FOA significantly improves facial symmetry, which helps your child feel more confident in their appearance.
- Most children will not remember the surgery, especially if performed in infancy.
- Scars are usually hidden under hair, making them barely noticeable as your child grows.
Social and Emotional Support
- As your child enters school-age years, they may have questions about their surgery. Providing age-appropriate explanations can help them understand and feel proud of their journey.
- Connecting with other families who have gone through FOA can provide valuable support for both you and your child.

Support for Parents and Patients
The journey through FOA is not just a medical process—it’s an emotional and psychological experience for both the child and their family. Parents often face a mix of anxiety, stress, and uncertainty when navigating the diagnosis, surgery, and recovery. While FOA has excellent outcomes, the process can still feel overwhelming.
This section will focus on how parents can support their child, manage their own emotions, connect with helpful resources, and prepare for life after surgery.
Coping With the Emotional Impact of Fronto-Orbital Advancement
Range of Emotions
Many parents experience a range of emotions after their child’s craniosynostosis diagnosis:
- Shock and fear: “What does this mean for my child’s future?”
- Guilt: “Did I do something to cause this?”
- Anxiety about surgery: “What if something goes wrong?”
- Relief after treatment: “I’m so glad we caught this early.”
These feelings are completely normal. The key is to acknowledge them and seek support when needed.
Ways To Manage Parental Anxiety
Many parents experience a range of emotions after their child’s craniosynostosis diagnosis:
- Shock and fear: “What does this mean for my child’s future?”
- Guilt: “Did I do something to cause this?”
- Anxiety about surgery: “What if something goes wrong?”
- Relief after treatment: “I’m so glad we caught this early.”
These feelings are completely normal. The key is to acknowledge them and seek support when needed.
- Educate yourself: Understanding the procedure helps reduce fear of the unknown.
- Talk to your child’s medical team: Ask questions, no matter how small.
- Lean on family and friends: Accept help with childcare, meals, or errands.
- Connect with other parents: Online support groups and local meetups can provide reassurance.
Remember: You are not alone—many families have gone through this, and there is a community ready to support you.
Preparing Your Child Emotionally
You can help your child by providing not only physical but also emotional support. Here are some things you can do to make your child comfortable, both before and after surgery.
For infants and toddlers:
- Infants won’t remember the surgery, but providing a calm and reassuring presence helps.
- Stick to routines as much as possible before and after surgery.
- Bring a favorite blanket or stuffed animal to the hospital for comfort.
For older children (2+ years):
- Use simple, positive language:
- “The doctors are going to fix your head so it can grow big and strong.”
- Role-play with a toy doctor kit to make medical settings feel less scary.
- Read sections about going to the hospital to help your child understand the process.
Pro tip: Children take emotional cues from their parents—staying calm and positive will help them feel safe.
Finding a Support System
Connecting with others who have been through FOA can be incredibly helpful.
Online Support Groups and Communities
- Cranio Care Bears is a nonprofit organization that provides care packages and support for families.
- The Children’s Craniofacial Association offers resources and advocacy for craniofacial conditions.
In-Person Support and Local Networks
- Ask your hospital or craniofacial team if they have support groups or local meetups.
- Some hospitals offer parent mentoring programs where families can connect with others who have gone through FOA. Hearing success stories from other families can be incredibly reassuring.

Navigating Financial and Insurance Considerations

Insurance and Coverage Tips
Surgery is expensive, and the financial burden can be stressful. However, FOA is considered medically necessary, meaning insurance typically covers most, if not all, of the costs.
- Call your insurance provider: Ask about coverage for surgery, hospital stays, and helmet therapy (if needed).
- Request preauthorization: Some insurance plans require approval before covering FOA.
- Ask about financial assistance: Many hospitals offer payment plans or financial aid programs.
- Save all medical bills and receipts: These may be useful for reimbursement or tax deductions.
Organizations That Offer Financial Help
- UnitedHealthcare Children’s Foundation provides medical grants for families in need.
- The HealthWell Foundation helps cover out-of-pocket costs for pediatric procedures.
- Some local charities and children’s hospitals offer grants or assistance for craniofacial surgeries.
Pro tip: A hospital social worker can guide you through financial options and paperwork.
Life After Fronto-Orbital Advancement: What To Expect Moving Forward
Once your child has recovered sufficiently from the surgery, their life will gradually return to normal. Here are some things you can expect during this phase.
Returning to Normal Activities
- Most children resume normal activities within a few weeks after surgery.
- Daycare and school: Check with your surgeon about when it’s safe for your child to return (usually within a month).
- Sports and rough play: Avoid contact sports until your child is fully healed (about three to six months post-op).
Answering Questions From Others
- Some people may ask questions about your child’s surgery or scar. Having a simple, prepared response can help:
- “They had surgery to help their head grow properly.”
- “It was a medical procedure, and they’re doing great now!”
- Over time, the scar will fade and be hidden by hair growth.
Final Thoughts on Support and Moving Forward
- Parents need support, too. Don’t hesitate to seek emotional help if you need it.
- Your child will grow up happy and healthy, and the experience of FOA will become a distant memory.
- You are not alone—many families have gone through this journey and are here to support you.
Future Directions
and Innovations in
Fronto-Orbital Advancement Treatment
FOA has been a gold standard treatment for craniosynostosis for decades, and advances in technology and surgical techniques continue to improve outcomes. As researchers develop minimally invasive approaches, biomaterials, and computer-assisted planning, the future of craniosynostosis treatment is evolving rapidly.
This section will explore the latest innovations in FOA and skull reshaping, including:
- Advancements in surgical planning (3D imaging and virtual simulations)
- New surgical techniques (robotics and endoscopic refinements)
- Alternative approaches (stem cell research and non-surgical options)

3D Imaging and Virtual Surgical Planning

Traditionally, craniosynostosis surgery has relied on surgeons’ experience and intraoperative decision-making, but modern advances in 3D imaging are revolutionizing preoperative planning.
How 3D Technology Is Changing Fronto-Orbital Advancement
- Detailed presurgical simulations: Surgeons can now use 3D CT scans to create a virtual model of a child’s skull, allowing them to digitally plan bone cuts and reshaping before surgery.
- Custom cutting guides: Using 3D printing, patient-specific cutting templates can be created, ensuring precise bone removal and reshaping.
- Improved surgical accuracy: Virtual planning reduces guesswork in the operating room, leading to more predictable and symmetrical outcomes.
Benefits for Parents and Patients
- More predictable results: Surgeons can show parents a before-and-after simulation of their child’s skull.
- Reduced surgery time: Less time spent making decisions in the operating room means shorter procedures and faster recovery.
Many leading hospitals now routinely use 3D surgical planning for complex craniosynostosis cases.
Robotics and Augmented Reality in Fronto-Orbital Advancement
Robotic-assisted surgery and augmented reality (AR) visualization tools are being explored to further improve surgical precision and safety.
Robotic-Assisted Cranial Surgery
- Some hospitals are testing robotic systems to assist in bone cutting and reshaping.
- Robotic precision reduces human error, especially in delicate areas such as the orbital bandeau (eye sockets).
Augmented Reality for Surgeons
- Surgeons can overlay 3D images onto a patient’s skull in real time, helping them visualize bone movements before making cuts.
- AR technology improves depth perception and accuracy, especially for complex asymmetries.
While still in early research stages, robotic-assisted and AR-guided FOA may become more widely available in the coming years.

Advances in Endoscopic Fronto-Orbital Advancement and Helmet Therapy

Endoscopic FOA has gained popularity in the field of craniofacial surgery for younger infants, and newer advancements are further refining this minimally invasive approach.
Improvements in Endoscopic Fronto-Orbital Advancement
- Less invasive techniques that require smaller incisions are being developed to further reduce surgical trauma.
- Better helmet designs are improving postsurgical reshaping, making endoscopic FOA a viable option for more cases.
- AI algorithms are being studied to predict skull growth patterns, allowing for customized helmet adjustments.
The future of endoscopic FOA may involve AI-powered helmet therapy, reducing the need for multiple adjustments.
Regenerative Medicine and Stem Cell Research
One of the most exciting frontiers in craniosynostosis treatment is the potential for biological approaches to replace or modify traditional FOA.
Can We Treat Craniosynostosis Without Surgery?
Scientists are exploring stem cell-based therapies that could:
- Prevent premature suture fusion by modifying bone growth signaling pathways
- Stimulate normal skull growth without the need for bone removal
Gene therapy research is also investigating ways to alter the molecular signals that cause craniosynostosis, potentially leading to nonsurgical treatment options in the future.
While these approaches are not yet available, they represent a promising area of research that could change the way craniosynostosis is managed in the next few decades.
Personalized Medicine and AI in Fronto-Orbital Advancement Treatment
The future of FOA may involve personalized treatment plans based on a child’s unique genetic profile and skull growth pattern:
- AI-driven algorithms can analyze thousands of craniosynostosis cases to predict the best surgical approach for each child.
- Genetic screening may help identify high-risk cases earlier, allowing for timely interventions.
- Custom biomaterials (such as 3D-printed bone implants) could eliminate the need for traditional bone reshaping.
As these technologies continue to develop, FOA may become even safer, faster, and more precise.

The Future of Fronto-Orbital Advancement:
What Parents Need To Know

- Advances in 3D imaging and robotics are making FOA more precise and efficient.
- Endoscopic FOA is being improved, making it an option for more infants.
- Stem cell and gene therapy research could lead to nonsurgical treatments in the future.
- AI and personalized medicine will help tailor treatments to each child’s unique needs.
While traditional FOA remains the standard of care today, these innovations are paving the way for a future where craniosynostosis treatment is even safer, more effective, and potentially non-invasive.
Frequently Asked Questions
Will my child have a visible scar after FOA?
- Traditional open FOA: The incision is made across the scalp from ear to ear, but it follows a zigzag or wavy pattern to help hair grow over the scar.
-
Endoscopic FOA: This surgery requires two small incisions (1-2 centimeters each), which usually become almost invisible over time.
Good news: In both cases, hair typically regrows fully, making the scar hard to see within a few months.Will my child need another surgery in the future?
For most children, FOA is a one-time surgery. However, additional procedures may be needed in some cases, including:
- Mild residual skull irregularities: Some children may develop minor asymmetries, but these are often not noticeable enough to require another procedure.
- Recurrent craniosynostosis (rare cases): In very rare instances, the skull bones re-fuse abnormally, requiring a second surgery.
- Syndromic craniosynostosis cases: Children with conditions such as Apert or Crouzon syndrome may require additional craniofacial surgeries as they grow.
For nonsyndromic cases, FOA is usually the only surgery needed.
How long does it take for my child’s head shape to look “normal”?
- Traditional open FOA: The results are immediate—the forehead and eye sockets are reshaped during surgery, and swelling resolves within a few weeks.
- Endoscopic FOA: The results develop gradually over 6-12 months, as helmet therapy helps guide skull growth.
The final results can take six months to a year to stabilize fully.
How painful is the recovery process for my child?
Most infants experience only mild to moderate discomfort, which is well controlled with pain medication.
- First 48 hours: Some fussiness due to swelling and anesthesia effects is normal.
- First week: Pain levels decrease significantly, and most infants return to normal behavior.
Many parents are surprised by how quickly their baby bounces back!
How long will swelling and bruising last?
- Swelling peaks at 24-48 hours after surgery.
- Most swelling resolves within seven to ten days.
- Any remaining bruising fades over two to three weeks.
Temporary eye swelling (causing the eyelids to close) can occur, but this resolves on its own within a few days.
Does helmet therapy hurt my baby?
No, helmet therapy is painless. The helmet applies gentle, consistent pressure to guide skull growth over time.
Most babies adjust within a few days and don’t mind wearing it.
Key to success: Parents must ensure their child wears the helmet as prescribed (23 hours per day) for the best results.
How long before my child can return to normal activities?
- Returning home: Most babies go home within one to five days (depending on surgery type).
- Eating normally: Children typically start eating normally within 24-48 hours.
- Tummy time: Supervised periods of tummy time can resume after two to three weeks.
- Daycare/school: Most children return within two to four weeks.
- Contact sports: These activities should be avoided for at least six months.
What are the biggest risks of FOA?
Like any surgery, FOA has risks, but serious complications are rare. Possible risks include:
- Blood loss: Some infants need a blood transfusion, especially with open FOA.
- Infection: Surgery-related infections can be prevented with proper wound care and antibiotics.
- Swelling-related complications: These complications are temporary and resolve naturally.
- Bone resorption (rare): Some bones may not heal perfectly, but this is uncommon.
Most children recover without complications and go on to develop normally.
Can FOA change my child’s personality or brain function?
No, FOA does not change your child’s personality, intelligence, or brain function.
- The brain is not touched during FOA—only the skull bones are reshaped.
- If anything, FOA helps ensure normal brain growth, preventing pressure-related complications.
Your child will be the same happy, playful baby—just with a properly shaped head!
How do I know if FOA was successful?
Surgeons consider FOA successful if:
- The forehead and eye sockets are positioned normally.
- The skull has enough space for brain growth.
- There are no signs of re-fusion or complications.
Most children never need additional interventions and go on to lead completely normal lives.
What should I do if I’m still worried about my child’s progress?
- Attend all post-op follow-ups with your child’s surgical team.
- If you notice any concerns (swelling, changes in behavior, skull shape irregularities), contact your surgeon immediately.
Your child’s medical team is there to support you every step of the way.
Key Takeaways From the Fronto-Orbital Advancement Journey
Diagnosis and need for FOA
- Craniosynostosis is a skull growth disorder caused by the premature fusion of cranial sutures.
- FOA is needed for frontal suture involvement (unicoronal, bicoronal, or metopic craniosynostosis) when skull and facial asymmetry is significant.
- Early diagnosis is important—endoscopic FOA is only an option for infants under 4-6 months.
Choosing the right surgical approach
- Traditional open FOA is best for older infants (6-12 months) and severe cases, providing immediate reshaping.
- Endoscopic FOA is a minimally invasive option for younger infants but requires helmet therapy for 6-12 months.
- Both approaches are highly effective, and your surgeon will help determine the best option based on your child’s age and skull shape.
Preparing for surgery
- Preoperative tests (imaging, bloodwork) ensure your child is healthy for surgery.
- Pack essentials for the hospital stay, including comfort items, snacks, and extra clothes.
- Prepare emotionally by educating yourself and connecting with support groups.
Surgery and immediate recovery
- Open FOA takes three to five hours, while endoscopic FOA takes one to two hours.
- Swelling peaks within 48 hours but improves significantly within one to two weeks.
- Most children are back to normal activities within a month.
Long-term outcomes and follow-up
- Skull growth continues normally after FOA, with regular follow-ups to monitor progress.
- Scars fade over time and are hidden by hair growth.
- Most children never need additional surgery and go on to lead healthy, normal lives.
Actionable Steps for Parents Moving Forward
- Stay informed: Keep learning about your child’s condition and treatment options.
- Trust your child’s medical team: Ask questions and communicate any concerns.
- Prepare emotionally and practically: Build a support system, plan logistics, and focus on a positive recovery experience.
- Follow post-op care instructions carefully: Proper incision care, activity restrictions, and (if applicable) helmet therapy compliance are crucial for the best outcome.
- Celebrate milestones: Every step forward in recovery is a victory.

Final Words of Reassurance
- You are not alone. Many parents have walked this path before, and with modern surgical techniques, your child has a bright and healthy future ahead.
- Your child is resilient. While FOA may seem like a big procedure, children recover faster than you expect, and most won’t even remember the surgery.
- FOA is life-changing, but it’s just one moment in your child’s journey. Soon, the surgery and recovery will be a distant memory, and your child will be thriving.
- You are doing an amazing job as a parent. Your love, support, and strength are exactly what your child needs to get through this.